The Listen, Believe, Affirm project came out of our work with the Centre of Expertise on child sexual abuse (CSA Centre). With their support, we carried out a survey across Change Grow Live to understand the level of skills and knowledge around child sexual abuse. We discovered that all of the tools were there – it was just a question of making sure those conversations happen. We needed to ensure that our staff felt comfortable and supported to ask the right questions, and that people were given the space to answer openly.
We had the opportunity to bring something to light that’s so rarely spoken about. We ask so many personal questions of people as a part of their support with us – why not ask them if they’ve experienced childhood sexual abuse?
Our first step was to train a series of practice leads to act as our organisational experts on psycho-educative work, myth busting, and how to build confidence and communication with people who’ve experienced childhood sexual abuse. Since then we’ve continued to build on this work and embed our learnings across the organisation. We’ve created accessible learning tools and run national conversation sessions to bring together voices of staff, experts, and people with lived experience of childhood sexual abuse. Through joint working with the Victim Support charity, we’ve carried out free online training for more than 800 of our staff and volunteers.
As the work began to take shape, the project became Listen, Believe, Affirm because those are the things we were hearing that people wanted. Not everyone wants extra support or a specific intervention based on their experiences – people just want to be asked the question and be heard, and to have their experience validated. Then they can make the decision that’s right for them.
We want to move towards a whole-person approach that considers all the factors in someone’s life. It’s about creating the conditions where people feel safe and where their substance use is seen as a symptom of trauma instead of a lifestyle choice. We’ve had people tell us that they’d never really discussed their experiences before, and that their lives might have been very different if someone had just asked them, and acknowledged what had happened to them.
Normalising the conversation around childhood sexual abuse is an important step in helping people feel comfortable linking past experiences to their current selves. And that process of normalising the conversation includes the conversations we are having as an organisation. By asking the right questions we can empower people to make the changes they want.
Ellie Reed is head of social work and Nicola Wendel is national CSE lead at Change Grow Live.
————–
Change Grow Live’s services work with so many people who have experienced trauma, including sexual abuse as a child. We know that childhood sexual abuse can be a contributory factor in problematic drug and alcohol use in adulthood, but there’s still so much stigma around discussing it openly.
It’s something that people may never have been asked about, or even felt comfortable to talk about. There’s a lot of fear across professionals – if they ask the wrong question, will they bring something up and make things worse?
Three ‘semi-synthetic’ cannabinoids (SSCs) have been identified on the European drug market over the last year, says EMCDDA, which may ‘signal the first major new change in the market for “legal” replacements to cannabis since Spice-type products (containing synthetic cannabinoid receptor agonists) emerged in Europe just over 15 years ago’.
The agency has issued a new report on hexahydrocannabinol (HHC), which is synthesised from cannabidiol (CBD) from cannabis plants, and related substances. HHC was identified in Europe in May last year, although it has been mentioned in scientific literature as far back as 1940. EMCDDA has been monitoring it as an NPS for the last six months.
HHC is sold openly in a range of products
HHC is not controlled in most European countries, although identifications have been reported by 20 EU member states as well as Norway, and the drug has also been found on sale in the US. Two more SSCs, HC acetate (HHC-O) and hexahydrocannabiphorol (HHC-P), have also since been identified in Europe, says EMCDDA.
HHC appears to have ‘broadly similar’ effects to THC, the main psychoactive substance in cannabis, the agency states. The drug is currently sold openly as a cannabis alternative in ‘a range of highly attractive branded and unbranded products’, including edibles, oils, vape pens and e-liquids.
The pharmacological and behavioural effects of HHC in humans have not been studied, although ‘recent anecdotal reports from consumers indicate that its effects might be similar to that of cannabis’, says EMCDDA, with the products’ marketing making comparisons to cannabis and THC.
‘The abuse liability and dependence potential of HHC have not been studied,’ the document says. ‘Data from pharmacological and behavioural experiments with several animal species as well as in vitro studies indicate that HHC shares the pharmacological mechanism of action of the structurally related THC suggesting that it may have abuse liability and dependence potential in humans.’ New consumers – including young and inexperienced people – may be attracted by its legal status, EMCDDA points out, along with its ease of access in high street CBD and vape shops.
Philip Breslin, on behalf of Adfam, explores why so many children are missing out on early help.
In January the Government released its annual adult substance misuse treatment statistics for 2021 – 2022. The figures mostly showed little change from the previous year and responses from Local Government, NHS providers and charities struggled to find anything new to say. They broadly welcomed an increase in the number of people seeking treatment for alcohol, and generally highlighted the many continuing challenges faced by the sector. It was not headline grabbing stuff.
Yet there is a line in the report that really should have caught everyone’s attention, It relates to the nearly 50,000 children whose parents (or other adults living with them) had entered substance misuse treatment in 2021/22. It simply says, “Sixty-five per cent of children of people starting treatment were receiving no early help.”
It’s worth reading that line again because it is a startling figure. Put another way; over 32,000 children were receiving no structured support despite the fact that they had a parent with a problem so serious that it led them into clinical substance misuse treatment.
The impact of parental substance misuse is well known. Decades of research by Adfam and others have demonstrated the range of difficulties that young people face when a parent misuses drugs or alcohol.
In a recent review by the Early Intervention Foundation (EIF) the negative impact on children is extensively evidenced (‘What works to improve the lives of England’s most vulnerable children’. May 2022). EIF found harms arose even where the parental drug or alcohol use was below the threshold for dependent use. These included heightened …”risk of internalising and externalising behavioural problems in childhood and substance use problems in adolescence and adulthood.” The report further points out that parental substance misuse is …”a key risk for child maltreatment…” and …”is consistently implicated in over one-third of serious case reviews.”
We know people rarely seek or receive structured substance misuse support at an early stage. By the time they enter a clinical drug or alcohol setting they have often been using problematically for many years.
So why are so many children missing out on basic early help? We know this is help that can make a real difference, including identifying where there are more serious risks. It is help which the same Government report asserts is provided to children and their families “as soon as problems emerge”. That is exactly what is needed. Sadly for most children with a parent entering drug or alcohol treatment, it’s just not happening.
This blog was originally published by Adfam. You can read the original post here.
DDN magazine is a free publication self-funded through advertising.
We are proud to work in partnership with many of the leading charities and treatment providers in the sector.
Premier League football clubs have ‘collectively agreed to withdraw gambling sponsorship from the front of clubs’ matchday shirts’, according to an official statement. This makes it the first sports league in the UK to ‘take such a measure voluntarily in order to reduce gambling advertising’, it says. The agreement will begin at the end of the 2025-26 season.
Removing short-front gambling sponsorship will be a ‘first step’ (Pic by Nick from Bristol, Wikimedia Commons)
The move follows extensive consultations between the league, its clubs and the Department for Culture, Media and Sport (DCMS) as part of the government’s ongoing review of gambling legislation. The Premier League is also working with other sports on the development of a new code for responsible gambling sponsorship, it says. Eight Premier League clubs currently have shirt-front gambling sponsors, including Everton, Fulham, Leeds, Newcastle and West Ham.
Sports sponsorship is one of the most contentious areas to be covered in the forthcoming Gambling White Paper, publication of which has been consistently delayed. It was last slated for publication last summer, and while many people were expecting it to be finally published at the beginning of this month (DDN, April, page 4), an official publication date has still yet to be announced.
The charity Gambling With Lives – which was set up by families bereaved by gambling-related suicide – said that while the move to voluntarily withdraw shirt-front gambling sponsorship was a ‘welcome first step’, the ‘nation expects the government to do much more than this, and soon’.
Germany’s plans to legalise cannabis for recreational use have been revised following discussions with EU officials. The proposal to allow the drug to be sold across the country in licensed specialist shops has now been scaled back to a set number of pilot areas for the next five years.
Adults will still be allowed to grow up to three plants for personal use but selling the drug through licensed shops will be carefully controlled.
Adults will still be allowed to grow up to three cannabis plants for personal use and possess up to 25g penalty-free, but will only be able to obtain the drug from licensed shops as part of a regional pilot project, health minister Karl Lauterbach announced. Germany’s government had agreed this after talks with the EU Commission, he said, although the aim remained to control quality, curb the black market, prevent the sale of contaminated drugs and ensure the ‘best possible protection for minors and health for consumers’.
Cultivation in non-profit associations or ‘cannabis clubs’ will also be allowed nationwide, provided membership is limited to a maximum of 500 people who are over 18 and resident in Germany. While there will be a general ban on advertising for the associations, ‘factual information is acceptable’. Specialist shops will then be established on a regional and time-limited model to allow the effects of a commercial supply chain on health, the black market and youth protection to be evaluated. Germany previously legalised cannabis for medical use in 2017.
Marco Buschmann: Time for a new approach that allows more personal responsibility. (Pic: Rob75, Wikimedia Commons)
The restrictive approach to cannabis in Germany had failed, added justice minister Marco Buschmann. ‘The prohibition of cannabis criminalises countless people, pushes them into criminal structures and ties up immense resources at the law enforcement agencies. It’s time for a new approach that allows more personal responsibility, pushes back the black market and relieves the police and prosecutors.’
The non-commercial supply models of home growing and not-for-profit associations avoided the ‘risks of over commercialisation’, said Transform, as well as the emergence of ‘Big Alcohol/Tobacco’-style monopolies and potential for ‘corporate capture’ of the policy making process. ‘On the other hand the absence of a regulated retail market inevitably means legal availability will be restricted and slower than it might have been – in turn meaning that the illegal market (and associated problems) will take longer to be eroded.’
Canada became the first G7 country to legalise and regulate recreational cannabis in 2018, with adults able to legally buy and possess up to 30g of the drug (www.drinkanddrugsnews.com/cannabis-becomes-legal-in-canada). The move has proved highly divisive, however, with critics claiming that the price and quality of the legal and taxed drug has meant its impact on the black market has been limited.
The Hep C Drug Treatment Provider Forum has been selected as the winner of the Best Healthcare Analytics Project for the NHS at the HSJ Partnership Awards 2023.
The Hep C Drug Treatment Provider Forum is a partnership of drug treatment providers, which includes Humankind, hosted by Gilead pharmaceuticals to collectively promote and manage hepatitis C provision among drug services nationally. The partnership’s ultimate aim is to work together to eliminate hepatitis C and the award has recognised its outstanding dedication to improving healthcare and effective collaboration with the NHS. Other partners include The Hepatitis C Trust, NHS England, NHS Addiction Providers Alliance, Change Grow Live, Forward Trust, Turning Point, WDP, and We Are With You.
Winners in a total of 21 outstanding categories, were announced during a ceremony at Evolution London, on 23 March 2023, hosted by comedian, Joel Dommett. Over 900 guests attended the event, bringing together national healthcare leaders and professionals from the NHS, public and private sectors. A total of 141 finalists were celebrated on the evening.
The Health & Care Act cites collaboration and partnership working as the key success factor for the future sustainability of the NHS. The HSJ Partnerships Awards are therefore not just a celebration of success stories but also a platform to shape the future of our integrated health and care system.
The prestigious award programme, now in its sixth year, recognises and honours the most effective partnerships, innovative projects and collaborations in the UK health system. A light has been shone on The Hep C Drug Treatment Provider forum and Humankind’s role in strengthening the healthcare system through the Award.
The judging panel was comprised of a diverse range of highly regarded figures across the NHS and wider healthcare sector.
Deborah Moores, national hep C coordinator at Humankind, said: “Together, national hep C coordinators have worked tirelessly to boost testing numbers far above levels prior to the pandemic and refused to take their feet off the gas to keep things moving.
“Recording accurately to reflect activity is always a challenge but by working together with a consistent approach. Four criteria were set to determine elimination, and a data system was created to be able to monitor progress against the agreed criteria. We now have accurate data that we can cross reference with other data streams and use to support services towards the goal of elimination.
“Winning the HSJ award for our work with data analytics has been the icing on the cake and will help to drive all services towards the elimination finish line. It is a true privilege to work with such a passionate group of individuals who are all working in competition every day but as one with the hep C elimination strategy.”
HSJ editor Alastair McLellan added: “The national healthcare sector faced innumerable pressures over the past 12 months, yet the standard and overriding positivity of the partnerships yet again this year highlights the enduring dedication to improving patient outcomes. So, we’re delighted that the Hep C Drug Treatment Provider Forum has been announced as winners in the category of Best Healthcare Analytics Project for the NHS at this year’s HSJ Partnership Awards 2023.
“The partnership stood out in an outstanding field of nominees, each showcasing the very best collaborations and innovations in the healthcare sector today. Well done – all credit to you and your team – you can be proud of all that you’ve achieved.”
The winners were selected following a rigorous two-stage judging process by a group of 90 judges ahead of the HSJ Partnership Awards 2023 awards ceremony. The full list of Winners and those Highly Commended for the 2023 HSJ Partnership Awards can be found at https://partnership.hsj.co.uk/winners-2023.
This blog was originally published by Humankind. You can read the original post here.
DDN magazine is a free publication self-funded through advertising.
We are proud to work in partnership with many of the leading charities and treatment providers in the sector.
The Forward Trust National Reunion was hosted at Conway Hall in London this year on the 14th of January.
It was originally scheduled to run in September 2022 but was postponed due to the passing of Queen Elizabeth II and subsequent period of national mourning. Forward Trust clients (past and present), including all our Forward Connect members, were invited along with friends and family, Forward staff members and other professionals.People came from as far as Wiltshire, Liverpool and Hull to attend the event – with free travel provided from the main community hubs for anyone who wished to attend.
Staff arrived at 9am to start setting up the registration desks and preparing the audio-visual and catering teams for the large turnout of people that were expected to attend the event. By 10am, the doors were ready to be opened, just in time for the coaches from East Kent and Hull. As people started to enter the venue, it became clear that the day was going to be a good one– how could it not be with so many people, and unlimited tea & coffee!?
Forward Trust CEO Mike Trace took the stage to welcome everyone and invite people to their seats. Mike spoke about the reunion being the celebration of people’s ability to change, which was perfectly highlighted by the day’s five main speakers: Melissa, Leon, Carol, Mike and Alistair.
Melissa and Leon spoke about their firsthand experiences of recovery and Carol spoke about her family’s experience of their son’s addiction and how they learned to heal. Mike and Alistair spoke about their time with The Forward Trust’s Enterprise support team, part of Forward’s employment directorate.
The event was hosted by the Forward’s very own Joshua Thetford (Forward Connect Coordinator) and Lyndsay W (Clouds Graduate 2022). The dynamic duo effortlessly introduced speakers to and from the stage with panache. Both felt it was a particular privilege to be able to oversee the clean-time countdown, which saw audience members in recovery stand up to celebrate their recovery and that of others around them.
Seeing people who had been sober for over 20 years stand side-by-side with people who were in their first weeks of recovery, celebrating and supporting one another’s achievements, bravery and hope was an utterly amazing experience.
As the morning progressed, there was time for a break. The atmosphere was electric, and the space filled up with hundreds of people chatting and sharing memories. When everyone came back to their seats, Hannah K took to the stage and sang, letting everyone know that she was celebrating her six-month sobriety milestone on the same day. She sang beautiful covers of Something in the Orange, She Will Be Loved and Hometown Glory – breathtaking!
For the first time at a Forward Trust Reunion the microphone was passed over to clients of the Enterprise service, a part of the organisation that supports people starting and building their own businesses. The speakers that took to the stage spoke about their own journeys through hardship and their drive for success in the face of adversity.
The open mic section followed and was particularly special, with many tributes read out for Ade Onilude, Forward’s Mentoring Programme Coordinator who sadly passed away in September 2022. The room was filled with passion as people spoke about their own experiences in recovery – some even called it the highlight of the event.
After lunch, it was over to Forward’s Recovery Support team to put on an afternoon of entertainment and games as part of the event’s winter-fete. There were games to play and sweet treats on offer from the ice cream, candy floss and popcorn carts. Forward Connect volunteers and staff helped to make sure people were well fed and entertained at the various stalls that were open: guess the teddy bear’s name and count the jellybeans, to find the buried treasure, hook a duck and tin can alley. Dotted throughout were stalls set up to promote the diverse services that Forward offers, with a special guest appearance from the Hep-C Trust, who came to do some onsite testing.
Once the ice cream had been eaten and all the prizes had been won, it was time to start slowing the event down as people got ready to board their coaches back home. A big shoutout to the crowd from Liverpool who stayed until the very end – waiting for their coach to arrive!
Over three-hundred-and-twenty people came to celebrate the many forms recovery takes within the services offered by The Forward Trust. It was an incredibly special day.
If you were unable to attend this year, don’t worry – our next national reunion will be taking place in January 2024, and we would love for you to join us.
This blog was originally published by The Forward Trust. You can read the original post here.
DDN magazine is a free publication self-funded through advertising.
We are proud to work in partnership with many of the leading charities and treatment providers in the sector.
New Vision Bradford is a new service to help people who have issues with alcohol and other drugs across the district.
The service, which starts on 3 April 2023, is a partnership between Humankind along with three local charities, The Bridge Project, Create Strength Group and Project 6, who have been offering support from their bases in Bradford and Keighley for many years.
New Vision Bradford has been commissioned by Bradford Metropolitan District Council and the NHS West Yorkshire Integrated Care Board through the Bradford District and Craven Health and Care Partnership.
Humankind Regional Director Lee Wilson, who will oversee the service, said, “We plan to build on the experience of our partners to make New Vision Bradford one of the most innovative and effective substance support services in England.
“We already have plans in place for treatment pathways and models that can help people achieve their goals and build better lives for themselves. We’ll be working closely with other partners in health and social care across the district and listening to the people we support to continually develop and improve what we have to offer”.
Sasha Bhat, Programme Director – Healthy Minds for the Bradford District and Craven Health and Care Partnership, added, “We recognise that providing compassionate and people-centred services to support people experiencing substance dependency is the best way to create long-lasting behaviour change.
“We’re delighted that this new service will help local people and do so in a way that is non-judgemental and at a pace that suits each individual. We want people to know that this service will be there for you in your recovery journey.”
New Vision Bradford will include a range of support including harm reduction, care coordination, clinical and therapeutic interventions. The service will also provide support for family members. New Vision Bradford will continue to work with people who become abstinent to help them create a healthy and meaningful life.
Reach Out is The Forward Trust’s online web-chat service, offering free, confidential support to anyone aged 16 and above who may feel isolated or overwhelmed by struggles with addiction, mental health and/or other challenges.
Our volunteer agents freely offer their time to help encourage individuals in accessing support, often signposting people to Forward’s community services. Our volunteers have a pivotal role, helping to capture motivation and encourage people to take the first step in getting help and support for drugs and/or alcohol issues. Our volunteer agents, who manage the web chat conversations, encourage new and former clients to self-refer by phone, email or drop-in to local community units. They also encourage people to use online referral forms where they exist for services.
The most common reason people contact Reach Out is to find someone to talk to. We are providing an invaluable service, helping people feel they are not isolated and alone with their struggles. During the last calendar year, Reach Out agents responded to 3,531 live chats or replied personally to the offline messages left when the service was closed.
During recent months, we have seen an increase in the number of people contacting us about substance misuse issues – the most common reason people got in touch was seeking support for their own drug and alcohol issues (on average 40%). However, the service is also being used by family members; agents often explore services of support for loved ones and listen to the issues of concern for the family member, encouraging them to seek support for their own understanding and psychological health and wellbeing.
The Reach Out team have been working hard to promote the service to the widest audience possible, with support from the communications team. Outreach has included linking in with universities to promote the service to their students, notably the University of Kent in Canterbury and Nottingham Trent University. Both have embedded information and links to Reach Out within their student well-being portals.
We are fortunate to have 15 volunteers who on average offer a three-hour shift weekly to respond to the live webchats. We have a good mix of skills within our volunteer team – we have many students who are gaining experience who work alongside volunteers with lived experience and want to give back. I personally can’t thank the Reach Out Volunteers enough as without their continued support the service simply wouldn’t run as effectively as it does. But we are always looking for more people to join the Reach Out team.
We currently offer Reach Out training for any existing Forward Trust volunteer who is interested in finding out more about Reach Out and web chat support, and the relevance this has for the people we support. There is no obligation to volunteer for Reach Out – this is a free training opportunity that you are welcome to attend.
If you are a current Forward Trust volunteer or staff member and are interested in attending a two-hour initial Reach Out Training Session delivered via Microsoft Teams, please contact Juliet Perschky.
This blog was originally published by The Forward Trust. You can read the original post here.
DDN magazine is a free publication self-funded through advertising.
We are proud to work in partnership with many of the leading charities and treatment providers in the sector.
Change Grow Live has published its Gender Pay Gap Report for 2022.
The people we exist to support are disproportionately affected by stigma, inequality, and prejudice. By taking action to make our society more equal and inclusive, we can make a real difference that is felt throughout our communities.
This difference can begin with the steps we take to improve our own organisation – including publishing our Gender Pay Gap Report for 2022, which you can read at the bottom of this page.
Understanding the gender pay gap
A gender pay gap is a measurement of the difference between men’s and women’s salaries within an organisation. It is different to equal pay which means men and women must be paid the same salary for the same work. This is a legal requirement and Change Grow Live complies with this legislation.
Reporting our gender pay gap is an annual legal requirement, but it is also an opportunity for us to learn and understand where we can make improvements that live up to our values of being open, compassionate and bold.
Our gender pay gap
A snapshot of our gender pay gap was taken on 5 April 2022 and our Gender Pay Gap Report 2022 was put together from the data collected.
Our gender pay gap by median average is 6.1% in favour of men, which is an increase of 2.9% since the same time last year.
There has been an increase in the gender pay gap, however there are clear signs that women have real opportunity for progression within Change Grow Live. We have seen an increase in the number of women employed in our senior roles.
Following a number of successful recruitment campaigns we have increased the number of women recruited in frontline roles. This his contributed to our gender pay gap.
Addressing our gender pay gap
Since we released our last Gender Pay Gap Report, we have taken a number of significant steps to address differences in pay including a significant cost of living award benefiting those on the lowest salaries. You can find out more in our Gender Pay Gap Report by following the link at the bottom of this page.
Throughout 2023 we will continue to build on the steps outlined in our Gender Pay Report and address the underlying causes of our gender wage gap.
Simone James, our Director of Equality, Diversity and Inclusion, said, “Our values are being open bold and compassionate. We’re proud to be a transparent and a learning organisation.
We want to share our commitment to creating a diverse and inclusive organisation Publishing our gender pay gap, as well as ethnicity pay gap information going forward allows us not only to learn from our own data, but to share the actions we are implementing with those who work with us.”
We pride ourselves on being an organisation that believes in people, regardless of their gender and background. We will continue to listen, to learn, and to make sure that we are an employer of choice for anyone who wants to make a difference in people’s lives.
You can read the full report and its findings by following the link below:
Handy naloxone pouches containing everything needed to make administration risk-free are a potential game-changer, says Alistair Bryant.
It would be cool if I can just explain our naloxone pouches and how we rolled them out. Everyone loves a backstory, right? So how did these pouches become a thing?
Chris Rintoul, our harm reduction and innovation lead, brought the idea to the table when he joined Cranstoun, and there’s a very real reason why these kits have been made the way they have. And that is that the reality of administering naloxone can sometimes be different to what you see in basic training.
Quite often naloxone administration happens in quite tough environments – alleyways or waste ground, cramped hostel bedrooms, or squats. It could also be dark, there could be glass on the floor, or even uncapped needles. All of these added risks for someone who is already responding to an opioid overdose can make the situation ten times harder.
So what we decided to do at Cranstoun was create a pouch that contained enough equipment to support the person administering naloxone in one of these risky situations. We decided that our pouches should contain a number of useful items, which are kept together for ease of access.
There’s a high-powered LED torch, a face shield for giving rescue breaths, instructions on how to administer naloxone and naloxone itself. We have two types of pouch, one containing nasal naloxone, and the other injectable.
One of the best things about the project was the big team effort. Chris Rintoul brought the original idea, our service commissioners supported the funding of the pouches and kits in a number of areas including Worcestershire. Ethypharm also kindly donated to wider distribution with 2,000 naloxone kits, which means 1,000 people will have access to a fully stocked pouch. Our Worcester peer harm reduction team, PACKS (peer-assisted community knowledge & support), helped get them all packed up for distribution – it was really special for PACKS to be involved in this as they had all lost someone to overdose and really enjoy being part of the bigger picture in preventing drug related deaths.
The passion the peer team bought to the table was quite amazing. You could really tell these pouches meant something personally to them. Without them, 2,000 would still be sat in boxes and I would be facing a telling off! So from me and all the people who now have a pouch, nice one PACKS – you did a mighty fine job on these!
I see these pouches as part of a shift towards ensuring that harm reduction is right at the forefront within Cranstoun services. We’re not only reducing harm by providing the ability to prevent overdoses, we’re also reducing the harm that our workers or other professionals could face when administering the naloxone. It was also the first project at Cranstoun Worcester where we worked with people who have lived experience and had them on complete equal footing as staff members, paid above the real Living Wage.
As always, we made sure we had some fun while we were packing the naloxone pouches – we’d get some pizzas in, get some music on and have a big factory line to get them packed. We also decided to make a TikTok video about them, and it was one of the videos that helped us go viral and reach over 1m views on our work. Such a high social media view count shows that harm reduction messages are very much here to stay – check out harmreduction_al on TikTok.
You can view more of Cranstoun’s naloxone and harm reduction videos on their site
It’s been incredibly refreshing to talk about keeping people who use drugs safe, and not having to focus solely on encouragement into abstinence or pushing them into recovery.
One thing we did notice when we were doing the naloxone training in public with the peer team was that sometimes people were interested in naloxone but didn’t have time to do the full training. So Deb from our Sutton service, the PACKS peer team and myself designed a Z-CARD which would contain all the key naloxone training information that could be given to someone with a kit. We know that if they read it they’ll have all the information needed to use the kit successfully.
Steve from the PACKS team came up with the quote we used – ‘I can’t save my friends, they’re gone. But you can save yours’. That always sticks with me and reminds me daily why we need to keep bringing harm reduction practice back. We need to bring care and compassion to the people who need it the most, wherever they are and whatever their need is.
Alistair Bryant is media and harm reduction content creator at Cranstoun.
The first comprehensive census of the field’s workforce provides a fascinating snapshot of a sector in transition.
Last month saw the publication of the first-ever national drug and alcohol treatment and recovery workforce census. Compiled by Health Education England (HEE) and the NHS Benchmarking Network (NHSBN), and based on impressive response rate of more than 80 per cent, the census covers the workforce for local authority-commissioned drug and alcohol services, local authority (LA) commissioning teams and LEROs in the year to 30 June 2022 – the first time the information has been gathered on anything like this scale.
The census report was commissioned as part of OHID and HEE’s drug and alcohol treatment and recovery workforce transformation programme in response to Dame Carol Black’s Independent review of drugs and the 2021 drug strategy, and will be used to help HEE work collaboratively with its partners to inform future planning and investment.
The Stats
There were almost 11,500 ‘whole-time equivalent’ (WTE) treatment provider staff and just under 400 commissioning staff in 2022, the document states. Almost half of the entire treatment provider staff were drug and alcohol workers, with the other half including 23 per cent working in service management and admin, 10 per cent in peer support and service user development, and 9 per cent who were nurses.
Three quarters of drug and alcohol services staff were working in the voluntary sector, followed by 15 per cent working in the NHS and 4 per cent in LA-delivered treatment. Three per cent were working in the independent or private sector, with 2 per cent working for LEROs.
Almost two thirds of the treatment provider workforce were female, with 84 per cent of staff on permanent contracts and 69 per cent working full time. Twelve per cent were unpaid volunteers, meanwhile, and there were 684 WTE peer support workers across the workforce.
Ten per cent of staff overall reported a disability, although this was lower for the NHS and LA sectors at 7 and 5 per cent respectively. The median percentage of staff who consider themselves part of the LGBTQ+ community was 2 per cent.
A quarter of the overall workforce were on salary band 5 (£22k-31k) with another quarter on band 6 (£32-39k). In the voluntary and independent/private sectors, however, around 80 per cent of the workforce were on band 5 or below, compared to approximately 65 per cent for the NHS and 57 per cent for LA-delivered treatment. More than 90 per cent of the alcohol and drug workers staff group were on band 5 or lower. Forty per cent of voluntary sector staff had been in post for less than a year, compared to 37 per cent of staff overall and just 17 per cent of LA-delivered treatment staff.
Watershed Moment
A striking element of the census – and one that represents a watershed moment in the sector’s development – is the growing presence of LEROs in the field, making it clear that Carol Black’s foregrounding of the importance of lived experience has been taken on board.
Although the document points out that some findings related to LEROs should be interpreted with caution because of the comparatively lower number of submissions, 46 per cent of the LERO workforce were in peer support and service user development roles, compared to 9 per cent of the treatment providers workforce.
Service managers, meanwhile, accounted for 17 per cent compared to 23 per cent for treatment providers. Seventeen per cent of the LERO workforce were volunteering or in unpaid roles, while almost 80 per cent were on band 4 or below (up to £26k). This compares with 12 per cent of treatment provider staff being unpaid or volunteers. At 34 per cent, a similar proportion of the LERO workforce had been in post for a year or less when compared to treatment providers.
Just over 40 per cent of the LERO workforce were on permanent contracts, and the same for fixed, while 17 per cent were on temporary contracts, whereas almost 85 per cent of staff at treatment providers were on permanent contracts. Just under 60 per cent of LERO staff worked full time, meanwhile, compared almost 70 per cent in treatment providers.
Older Workforce
Across the workforce as a whole, the percentage of staff from a Black/Black British ethnic minority background was between 5 and 9 per cent, compared to 4 per cent of the working-age population in England as a whole. However, the percentage who were Asian/Asian British was between 4 and 8 per cent, compared to 9 per cent of the working age general population. The sector’s staff meanwhile, is generally older than the working age population as a whole with higher percentages of staff in the 40-49 and 50-59 age bands.
The findings of the report have informed the soon-to-be-published Drugs and alcohol treatment and recovery workforce strategic framework, says HEE, and will also support the forthcoming comprehensive workforce strategic implementation plan.
Drug and alcohol treatment and recovery services: national workforce census at www.hee.nhs.uk
Drilling into the detail – The Data
There were 535 data submissions – 347 were from treatment providers, 165 from commissioners and 23 from LEROs. Most provider submissions were from voluntary organisations (78 per cent) followed by the NHS (18 per cent), and the independent/private sector (4 per cent). Submissions from LA commissioners included those reporting activity for commissioning staff only (72 per cent), those including activity for treatment staff employed by the LA (19 per cent) and those that sent submissions including both commissioning and treatment staff (9 per cent). By service type, most submissions were for community treatment and recovery services (69 per cent) followed by young people’s services (20 per cent), residential rehab (8 per cent) and inpatient detox (4 per cent).
Participation
Participation rates per sector were 89 per cent for local authorities, 81 per cent for treatment providers and 60 per cent for LEROs. ‘The percentage of LEROs who participated was based on a partial list and although this grew over the course of the project, remained incomplete,’ says the document, meaning the information should be viewed as ‘indicative rather than definitive’. The list of treatment providers also changed – expanding from lead providers submitting to NDTMS to also include submissions from sub-contracted services for a more comprehensive view.
Geography
The census received submissions from all sectors for all seven HEE regions – East of England, London, Midlands, North East and Yorkshire, North West, South East and South West. Most independent/private sector submissions were from the North West, and most submissions for LEROs were from London and the Midlands, although there was at least one for each region.
Workforce Transformation
Workforce transformation is a key function of HEE, to support the development of a workforce that’s responsive to change. ‘Workforce transformation is a process, driven by improving the way we recruit, retain, deploy, develop and continue to support the healthcare workforce, to meet the growing and changing needs of local populations – ensuring high quality care for the patients of today and the future,’ HEE states. ‘COVID19 in particular has shown us how imperative it is to have a skilled, flexible and resilient workforce, able to adapt quickly in times of crisis to deliver the best healthcare possible in a way that works for all.’
We talk about ‘the workforce’ and there are new strategies on the way – so it’s been interesting to look at the first census of its kind in England. It gives a snapshot of who we are – and shows that lived experience has become an important part of the workforce. The peer team distributing naloxone pouches (page 16) demonstrate the passion and connectivity that’s so important – and those with lived experience are involved in the project on an equal footing and paid properly.
But statistics don’t tell us about quality or the special attributes of so many in the sector. It takes specific skills to work responsively with people in a prison environment, helping to build a personalised plan for a safer future (p11). It goes beyond assessment and involves networking, joint-working and showing compassion and imagination in supporting those who find change difficult.
There must be many days when it feels too difficult, but the outcomes can’t just be measured on a spreadsheet. Working with child sexual abuse is equally complicated, but with specialist skills the results are life-changing (p10). Being responsive is central to the way we work, so Anna’s powerful perspective on mothers (p14) will give clear direction on where we must focus.
Mothers have been misunderstood, under-represented and ignored – it’s time to redress the balance, says Anna Millington.
I am a mother, a drug user, an activist, a researcher, a trainer and a professional. I’ve used drugs from the age of 13 – I was a problematic user when my child was young, I’ve been to prison on several occasions, been sentenced to various criminal justice orders and traversed through the whole spectrum of drug treatment. I also had my child put into the care of my mother for a period before regaining full rights.
During the last 15 years I’ve worked within the drug treatment sector at national level, with the government, academia and the probation service, and within prisons. I’ve been on the ground floor helping my peers voluntarily for a long time – I’m passionate about making sure there are effective ways out for people if they want it, and help and harm reduction if they don’t.
For the last eight years I’ve worked extensively providing harm reduction equipment and wide-ranging peer support to mothers who use drugs. Those in hiding and in fear, those with extensive needs who feel alone and trapped, unable to come forward. These mothers may not make up the majority of the using community, but they can be one of the highest-costing sectors societally, generationally, and economically. Providing what may be termed as high-risk support to this group is demanding, and has had both positive and negative outcomes, but I believe that risk is inherent in anything – including doing nothing at all.
Skewed System
Let me be clear before I continue – I think the work and focus on women by activists, peers, workers, managers, and leaders is fantastic. I’m not trying to diminish nor take anything away from that, because I champion the need in this male-dominated system to finally address us, listen to us and understand our needs, as well as adapt services and service provision.
However, if we’re going to fully embrace women and finally make major changes to include their needs in everything we do it’s impossible to discuss us in relation to the criminal justice system, harm reduction, drug treatment and recovery without including within that – as a priority – motherhood.
It’s clear this sector of our using community has continually been misunderstood, underrepresented, and constantly ignored unless under the guise of a misguided and ill-judged child protection rhetoric.
A tokenistic head nod when discussing ‘women’ generally without specifics of who we are and what we explicitly require as mothers, as part of a family unit, is not acceptable. It’s not just professionals that avert their gaze and interest from us either – recovery/peer community led projects do too.
Stern Judgements
We face harsh and complicated barriers when accessing harm reduction services, and we face sterner judgements and discrimination both societally and within professional and peer services. It’s almost impossible to be a drug using mother and for that to be okay in and of itself.
We can use drugs without this automatically causing harm to children. It’s not a given that risk and harm naturally follow from the use of drugs themselves. It’s often the lifestyle and the associated links that tend to be a problem. If services work from the belief that parental drug use is negative, that it equates to risk or harm or its ‘user representatives’ hold this belief then it’s most likely that they are incapable of addressing this topic adequately, logically, and impartially. Nor can they effectively and fairly represent, or proactively work with, this group. It’s doomed from the start.
We’re required to make superhuman leaps in the drug treatment system. We are punished if we don’t adhere to unrealistic goals within unrealistic time limits. We are expected to move quickly through a recovery journey that we cannot choose freely, without the appropriate support needed by us and our children and end up as a fully recovered person as defined by other people. We’re told what we must do, what way we must do it and when we must do it by. The consequences for failing any of this can be severe. It can lead to the loss of your children. I really want that to sink in for people. It’s a reality. Intentionally or not, the normal expectations and requirements for a person who uses drugs do not apply to us.
Outdated Terms
I had some input into the original Hidden harm work. Its title is as outdated as some of the content – using titles like ‘hidden harm’ for specific pieces of work or for specific workers has clear implications that you are saying from the start that there is harm. It’s hard to move forward positively from this point if it starts from a negative stance. The mothers I work with have told me that this type of thing is what immediately scares them – the title can put them off from engaging and it doesn’t really matter what people try to explain about the role or work. They’ve already mentally disengaged, run a mile, or remained hidden.
I think that a lot of the roles themselves are often positive, exciting and innovative, but may end up becoming under-used and tokenistic if we can’t get the people who need this the most to engage, or if the right workers who understand these intricate and often very demanding and challenging clients and issues aren’t employed.
Double Standards
I continually come across double standards and contradictions in relation to mothers who use drugs. We are often accused of putting our children at risk of harm and damaging them, but equally nothing appropriate or realistic is offered – no real tools or therapy are given, or real time invested to help mothers mitigate or deal with their issues. There are no strong cross links with children’s mental health services that may be able to provide the type of family therapy needed. We are then blamed and labelled as failures at motherhood when things go wrong, or we aren’t seen to comply.
We have complex needs which require complex treatment plans. We need specific and targeted medication and psychosocial help. We need this provided by people who understand the reality of our situations, who are both qualified and onboard with our struggle to come forward and access suitable, sustainable, effective harm reduction services and drug treatment. It’s possible. It can work, there can be a positive successful outcome. But it only happens when services and organisations are invested in really wanting to make it work. In thinking outside of the box.
Anna Millington established a non-funded, non-affiliated support network for mothers who use drugs. It seeks to work collaboratively with professionals – on its own terms. annaddition@gmail.com
We’re Not Going Away
Motherhood is for life, regardless of whether you have your child with you or not. Those whose children are not in their care appear to somehow lose their motherhood status.
Mothers in treatment who don’t have their children with them still require appropriate and specific psychosocial help around this. Where do we fit in? What is harm reduction for mothers? What does it look like? How can we identify and try to reduce the risk and harm if there is any? How would we assess it? Can we change the discourse and views on mothers who use drugs so it can instead be used as a motivating positive factor for engaging in treatment? Why is this not a topic with any real spotlight? Why is no one trying to answer these vital and important questions?
I think many organisations and services remain silent because they think it’s impossible to fix. But surely we should try to fix what we can. I don’t claim it’s easy, I just claim it’s needed. I’m not asking for the impossible. I’m not expecting there to suddenly and easily be some ‘eureka’ answers. What I am asking people to do is put it on the table. Discuss it, evaluate it, look at your way of working, service and organisation. It is time to stop ignoring us.
The call for action on prison failure is clear, as DDN reports.
There is an identifiable cohort of people responsible for prolific offending among those showing up in police stations and courts, Mike Trace, CEO of Forward Trust told the latest meeting of the All-Party Parliamentary Group on Drugs, Alcohol and Justice. ‘If we can identify, motivate and treat them, we can have a big effect.’
The Morgan Report (2014) had looked at effective approaches to crime prevention. We needed to apply that logic to prisons, he said, and look at motivating people not to reoffend.
Mike Trace, CEO of Forward Trust
A look back at recent history revealed a scattergun approach. Cranstoun’s release scheme and RAPt’s intensive abstinence-programmes had popped up in the 1990s and finally, at the beginning of the 21st century, there had been a good treatment budget. A specialist service was set up in every prison, with an expansion of both OST and abstinence-based treatment.
‘It all looked pretty rosy in 2010,’ he said, ‘but it all went wrong in 2012’ when drug treatment went from the Ministry of Justice to the Department of Health. ‘It wasn’t a bad decision to take it to health – but we lost all our learning,’ he said. There were new statistics, new priorities and new learning systems, with counselling, assessment, referral, advice and throughcare (known as CARATs) leading to a ‘quantity not quality’ system.
A vast amount of the target group got rushed interventions, said Trace – and the vast majority of the structured programmes in prisons were closed down. ‘Some were poor quality, but many were research-based and flying,’ he said. We had entered an era of decline and missed opportunities. Furthermore, ‘the wing drug dealers won massively in the 2010s’ with the expansion of markets, introduction of spice, and the pressure to use instead of engage. With drug markets now out of control, we had not created the environment where prisoners could go for treatment instead of using drugs in prison.
Dame Carol Black’s report represented a phase of refreshment, he said – a chance to come back from ten years of neglect. There was no underestimating the ‘awful challenge’ for prison staff, with ‘the nature of being a prison governor [being] to get through the day’. The bit of money would have to go a long way, as we were still faced with the same problems, with ‘services massively stretched’. But at least there was political attention and acknowledgement that things must change.
As criminal justice service manager at Humankind, Jessica Scott brought experience from a cluster of seven prisons in the North East, where the organisation had worked with its healthcare partner Spectrum and delivered psychosocial interventions.
Humankind Service Manager, Jessica Scott
‘It’s about reconnecting our men and women to health and their personal goals,’ she said. ‘Our services are about finding that glimmer of hope, and about clinical and non-clinical services working together, making sure there’s no break in support.’ Detox and therapies were available when people came into prison, to make sure they were well enough to have interventions, and there was planning around release that included carrying a naloxone kit.
‘We want to replicate in prison the options that people could have in the community,’ she said, including prescribing slow-release buprenorphine injections (which lasted a month and saved staff time as well as pharmacy visits) and providing a family service to create a strong network on release. Recruiting peer mentors had given an extra, and very valuable, level of support to recovery services, while resettlement workers looked at housing needs.
The demographic of different prisons had informed different initiatives – from a particular emphasis on harm reduction in a high-security environment, to care around hormones in a women’s prison, to an ‘Old Wise Lads’ mutual aid group in a prison with a population of over-50s. But throughout each estate, continuity of care was a real challenge, she said. ‘We need to look at our practice – and the gaps.’
Pete explained how, after leaving prison in 2000, he became trapped in a ‘cycle of failure’. He had treatment with methadone in prison, but once outside and faced with the same housing problems, he would be back on heroin, back to the police station, back to prison, back on a script. And so it continued.
‘There was no support between prison and community, nothing ever materialised at the gate,’ he said. ‘The first thing I wanted to do was celebrate with a drink… then crack and heroin.’ It was similar each time, beginning with sofa surfing at the dealer’s. ‘I’d think, what’s the point? It’s all I know. And it happened to many others I know.
‘There’s such a culture of picking on the vulnerable. I saw the spice culture escalate and it was pitiful. I knew someone who committed suicide with no hope of getting out. You get used to blocking out feelings – you can’t show vulnerability.’
In looking for solutions and hearing the varied experiences of the group, it was clear that no one thing worked for everyone. For some, it was 12-step communities, but you had to ‘want them to work’. For others it was a methadone detox, and the opportunity to feel better. Training and employment programmes had offered ‘massive therapeutic value’.
But the reality for so many prisons was that life inside and outside was a struggle. Men leaving the prison on a Friday with £80 in their pockets had to navigate the line of dealers’ shiny cars and the newsagent doing a brisk trade in Kestrel Super. The key factors that would offer the chance of a different outcome were housing, recovery and employment – but if any of them were missing there was little hope.
A change of direction for Pete came at the age of 42, when he ‘changed his mentality’ by focusing on restorative justice. Mike Trace believed that restorative justice was key – particularly when people were past their mid-20s, as it could be difficult to get through to them in the ‘gang stages’ when they were enjoying themselves and hadn’t yet hit the ‘misery stage’. Yet even though he’d listened to the ‘realities and difficulties of going against the flow’, we should never get to the position of saying someone can’t recover, he said. ‘Downview was once known as Brownview, because of all the heroin, but we created an oasis of calm, where 15 to 20 people lived differently.’ Similarly, living on a recovery wing in Wandsworth in the 1990s offered a very different experience. ‘Don’t be naïve,’ he advised – ‘but never say we can’t do it.’ DDN
Some Challenging Questions
‘Can we address the drivers of drug use in prison?’
Pete: ‘We’re never going to stop drug use. People are making money and will just come up with something else.’
‘Did you get any help with trauma?’
Pete: ‘Is it the right environment to address trauma? Going back to hostile wings? You want to open people up to explore their emotions? I had to be left alone – it was the only way to deal with it. I felt powerless. I was angry and frustrated, but I couldn’t show emotion as blokes would walk all over that.’
‘Is there a difference to how women respond to treatment – and are there any factors that affect recovery?’
Jessica Scott: ‘Women can be a support to the whole family. Give them power. They keep everything together but no one is looking after them. Women don’t get a lot of visitors – men get women to visit them. And they are often exploited.’
Last Friday, the 24th of March, the Social Interest Group Awards 2023 took place at Lift in Islington.
The event was attended by approximately sixty nominees and was a mix of staff, residents, and participants.
The event kicked off at midday with lunch, and it was brilliant to see everyone sitting around the tables chatting, eating, and sharing stories about their day and wondering if they were going to win an award.
At 1 pm, Greg Tythe, Director of Development, Marketing, and Communications, welcomed everyone to the event and introduced Gill Arukpe, Group CEO, to give an opening speech. Gill spoke about how proud she was of everyone in the group and of all the people nominated for the awards. She spoke about how challenging it was to choose the winners and how this year was the hardest yet because we have so many wonderful people doing exceptional things. She spoke about the achievements of the group as a whole and our aspirations to do more in this coming year to make a positive difference to those we support and to the wider community.
The winners were then announced amid claps and whoops and collected their awards and were personally congratulated by Gill.
There were also awards for people who have worked within their service for over 20 or 30 years. It was particularly great to celebrate Ned, who works in our maintenance team and is our longest-serving staff member. Ned has been with us for 33 years!
The award ceremony ended around 3:30 pm, and from the feedback gathered so far, all have said it was a fantastic event, which made them feel valued by the Group.
This blog was originally published by Social Interest Group. You can read the original post here.
DDN magazine is a free publication self-funded through advertising.
We are proud to work in partnership with many of the leading charities and treatment providers in the sector.
EDP has proudly supported people in the South West since 1984, and as a subsidiary of Humankind since April 2020. The two charities have worked closely together, with EDP drawing on Humankind’s national scale and expertise. As closely aligned charities, EDP will now take the next step in integration by merging fully into its parent charity on 1 July of this year.
Uniting the organisations will make us stronger and more sustainable. EDP’s Reach Dorset, Together Devon and wider services will become Humankind’s South West operational region, enabling us to serve the people of the South West even better, reaching a greater amount of people. There is no anticipated reduction in the overall number of roles.
As a national provider of support Humankind has services across England. We are proud to have supported over 90,000 people last year and that all our Care Quality Commission inspected services are assessed as ‘good’ or ‘outstanding’. The new South West operational region will be supported by Humankind’s core functions and will be able to draw on good practice, new models and resources from our other operational regions.
Paul Townsley, CEO of Humankind, said, “After three years of close partnership work, I’m delighted that Humankind will be welcoming EDP staff and services in July. I know both charities pride themselves on their partnership approach as well as their focus on, and belief in, the people they serve. We will ensure these values continue as part of EDP’s proud legacy in the South West.”
Penny Blackmore, CEO of EDP, added, “Working with Humankind as a subsidiary over the last three years has brought many benefits to EDP, so taking this next step feels very natural. Being able to deliver life changing recovery services with our trademark care and professionalism to more people in the South West is an exciting prospect, and one that we are now ready to take.”
This blog was originally published by Humankind. You can read the original post here.
DDN magazine is a free publication self-funded through advertising.
We are proud to work in partnership with many of the leading charities and treatment providers in the sector.
Three gambling businesses owned by the William Hill Group have been fined a total of £19.2m for social responsibility and anti-money laundering failures, the Gambling Commission has announced.
William Hill Organization operates more than 1,300 gambling premises across the UK.
The fines are £12.5m for WHG (International) Limited, which runs williamhill.com, £3.7m for Mr Green Limited, and £3m for the William Hill Organization, which operates more than 1,300 gambling premises across the UK. The £19.2m total exceeds the previous record fine of £17m for the Entain Group – which owns Ladbrokes.com, coral.co.uk and foxybingo.com – last year (www.drinkanddrugsnews.com/gambling-firm-hit-with-record-17m-fine).
The failures listed by the Gambling Commission include having insufficient controls to protect new customers and to ‘effectively consider high velocity spend and duration of play’, with one customer spending £23,000 within 20 minutes after opening a new account and another spending £18,000 within 24 hours – both without any checks.
Others include failing to identify customers at risk of gambling-related harm, failing to intervene early enough, and failure to apply a 24-hour delay before granting a credit limit increase. One customer lost almost £15,000 in just over an hour, another was allowed to immediately place a £100,000 bet when his credit limit had been set at £70,000, and another did not have a telephone interaction until his losses had reached almost £46,000. Operators also failed to obtain source of funds (SoF) evidence from customers staking large amounts of money, including one customer who staked almost £20,000 in a single bet and another who staked almost £277,000 – and lost nearly £25,000 – over two months.
Gambling Commission chief executive Andrew Rhodes
‘When we launched this investigation the failings we uncovered were so widespread and alarming that serious consideration was given to licence suspension,’ said Gambling Commission chief executive Andrew Rhodes. ‘However, because the operator immediately recognised their failings and worked with us to swiftly implement improvements, we instead opted for the largest enforcement payment in our history. In the last 15 months we have taken unprecedented action against gambling operators, but we are now starting to see signs of improvement.’
The government’s much delayed gambling white paper (DDN, March, page 12) is now expected to be published before Easter.
William Hill image: Acabashi, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia C
The Care Quality Commission (CQC) has rated WDP Harrow as ‘Good’ across the board.
The CQC inspectors highlighted that the team “treated clients with compassion and kindness” and that they “actively involved clients in decisions and care planning”.
The report shares that staff “developed holistic, recovery-orientated care plans informed by a comprehensive assessment” and that they “provided a range of treatments suitable to the needs of service users and in line with national guidance around best practice.”
The inspectors also identified areas of outstanding practice in the service, specifically:
WDP’s Capital Card scheme, where service users can earn points by attending appointments and engaging with treatment, and then spend their points on positive activities in their local community. Since the last inspection, staff had updated the scheme to include blood borne virus (BBV) testing and eye testing at the local clinic.
The service had a partnership with the local hepatology team, whereby clinicians offered liver function testing and then screened service users for referral into the hepatology pathway.
The report includes some exceptional feedback from service users. The inspectors reported that service users said the staff support is invaluable. They provided them with help, emotional support and advice when they needed it.
Service users described the service as a friendly, welcoming place where they are treated respectfully. Another service user said that the staff are good at listening, were non-judgmental and very encouraging in their recovery journey.
One individual described how the doctor ‘saved their life’ and went above and beyond.
Oasis Azeez-Harris, Interim Senior Public Health Commissioner for Substance Misuse and Sexual Health from Harrow Council, said: “In my experience, I have found it very easy and refreshing to work with WDP in that the management is flexible, responsive, innovative and always willing to try out new proposals to meet residents needs. As a commissioner, I am pleased to work with WDP and always look forward to jointly working together to respond to known and emerging identified needs of Harrow residents to ensure people’s lives are improved.”
Vanessa Duke, Area Director for WDP Harrow, added: “We are so pleased to have achieved a ‘Good’ rating from CQC, which acknowledges the hard work and commitment of our team in Harrow. The report showcases the compassion they have for our service users and the work they do to provide personalised high quality care to residents of Harrow.
“Being a part of a service users recovery journey is a great privilege and we are committed to working with them to continue to build on and develop the WDP Harrow recovery service. WDP have been delivering adult drug and alcohol treatment in Harrow since 2015 and we are proud of the strong working relationship we have built with our commissioners and we hope this partnership with continue to thrive to ensure the best outcomes for our service users.”
The Forward Trust has been awarded two major new contracts, helping even more people to change their lives for the better.
The Forward Trust are delighted to have won two new contracts to support people in Kent with education and training. These initiatives will allow us to provide tailored support to people who are either unemployed or have few qualifications, helping them to build a better future for themselves.
More detail on each of the contracts can be found below:
Multiply Scheme (East Kent)
The Multiply Programme is for adults living in Kent aged 19 and above who don’t already have a Level 2 Maths or equivalent (GCSE Grade C or above or Grade 4 or above). Forward are delivering the engagement parts of the programme in Thanet and also new numeracy courses in other parts of East Kent until December 2023.
Job Centre Plus (JCP) Dynamic Purchasing System (DPS), Thanet, Kent
Based on our extensive experience of delivering employability programmes including DWP Restart, Forward has secured a JCP DPS service in Thanet to support residents who are unemployed. The structured eight-week programme will provide one-to-one and group support with a focus on building skills and confidence in job search techniques, with the outcome of helping people back into sustainable employment and jobs. The programme will be delivered in Margate and Ramsgate. This programme will run until November 2023.
The government has announced that it will ban nitrous oxide, despite being advised by the ACMD not to do so.
Home Secretary Suella Braverman: ‘The British public are fed up with crime and nuisance behaviour.’
The much-anticipated move is part of a wider ‘anti-social behaviour action plan’ that also includes giving the police more powers to test for drugs on arrest.
Banning nitrous oxide will ‘send a clear message to intimidating gangs, that hang around high streets and children’s parks and litter them with empty canisters, that they will not get away with this behaviour’, the government states. The ACMD, however, had advised the government that the harms associated with the drug were ‘not commensurate with control under the Misuse of Drugs Act 1971’, and also warned that a ban would place ‘disproportionate burdens’ on its legitimate use in medical, industrial and commercial fields (www.drinkanddrugsnews.com/acmd-advises-government-not-to-ban-nitrous-oxide).
The action plan also expands powers for drug testing on arrest, allowing more people to be tested and more substances to be tested for – including MDMA and methamphetamine. At the moment only people suspected of committing certain offences can be tested in police detention without additional requirements, but the government says it will expand the range of ‘trigger offences’ to include crimes linked to violence against women and anti-social behaviour. It also states that it intends to tackle the practice of ‘cuckooing’ – where vulnerable people have their homes taken over for use by drug dealers – by looking into creating a new criminal offence.
‘The British public are fed up with crime and nuisance behaviour in their neighbourhoods inflicting misery on people,’ said home secretary Suella Braverman. ‘It has always been my priority to give police the powers they need to deliver a common-sense approach to cutting crime, which puts the law-abiding majority first, and that’s what this action plan delivers.’
Release Executive Director, Niamh Eastwood: ‘The government is ignoring its own experts.’
The decision to ban nitrous oxide has been condemned by Release, which points out that ‘no expert nor clinician appears to support the criminalisation of possession’. The move will ‘inevitably’ target young people, it adds, and deter them from seeking help if they need it. ‘The government is ignoring its own experts, in an attempt to out manoeuvre Labour as both of the main parties try to appear tough on drugs,’ said executive director Niamh Eastwood. ‘Nitrous oxide is a relatively safe substance, and possible health harms could be mitigated through a large-scale harm reduction campaign, educating people on how to stay safe. There is a much bigger risk associated with criminalisation, which impacts life opportunities including education and employment.’
Criminalising possession of the substance will increase both the health and social harms associated with it, added Transform’s senior policy analyst Steve Rolles, creating ‘new costs across the criminal justice system’. To reduce risks the government should instead direct resources towards education for vulnerable groups, he said, and restrict sales of larger cannisters that have no legitimate use.
A compendium of specialist alcohol and other substance services for people in minority ethnic groups or migrant communities has been launched by Manchester Metropolitan University in partnership with OHID.
The document was compiled via extensive online searches and through social media, with the team keen to ensure that peer-led services were included. Follow-up calls were then made to government bodies and other services. Available as an Excel spreadsheet, the compendium covers the entire UK and includes the specific cultural focus of each service and details of the support provided, along with referral pathways, contact details and costs, if applicable.
Prof Sarah Galvani: hoping to make the compendium a comprehensive resource
‘To my knowledge the compendium is the first of its kind,’ says Professor Sarah Galvani, professor of social research and substance use at Manchester Metropolitan University. ‘The uncomfortable reality is that there is very little out there. We are happy to share it and we would also be delighted to hear from anyone we have missed out or whose details are wrong.’
There was an estimated 13 per cent reduction in deaths and a 4 per cent reduction in hospital admissions ‘wholly attributable to alcohol consumption’ as a result of the implementation of minimum unit pricing (MUP) in Scotland, says a study by Public Health Scotland (PHS) and TheLancet in collaboration with the University of Glasgow. The estimated findings cover the period between MUP’s implementation in 2018 and the end of 2020.
MUP was found to be reducing deaths and hospital admissions
MUP had also reduced deaths and hospital admissions where alcohol ‘may be one of a range of causative factors’, the report states. A separate study from PHS and the University of Glasgow late last year found that MUP had led to a 3 per cent reduction in off-trade alcohol sales (www.drinkanddrugsnews.com/scottish-alcohol-sales-down-3-per-cent-since-mup).
According to the most recent National Records of Scotland statistics, however, deaths from ‘conditions caused by alcohol’ reached their highest level for more than a decade in 2021, at 1,245 (www.drinkanddrugsnews.com/scottish-alcohol-deaths-at-highest-level-for-13-years). The report’s study period doesn’t include 2021 but the document states that ‘the age-standardised rate of alcohol-specific mortality increased by 7 per cent from 2020 to 2021 in England, compared to 4 per cent in Scotland – it is therefore unlikely that the inclusion of mortality outcomes from 2021 would have altered our findings.’ There have been suggestions that COVID-19 ‘may interact with existing liver problems, and potentially increase vulnerability to those already at the highest risk of alcohol-related harms’, it adds.
Prof Jim Lewsey: confident that MUP was reducing alcohol health harms
The researchers state that they are confident that the reduction in health harms was the result of the introduction of MUP, rather than other factors. ‘Our approach compared what happened to alcohol health harms in Scotland with its neighbouring country, England, where MUP was not introduced,’ said professor of medical statistics at the University of Glasgow, Professor Jim Lewsey. ‘The methods we have used and the consistency of our findings with what was anticipated before MUP was introduced allow us to be confident that the reduction in alcohol health harms is because of the MUP intervention.’
The study estimates that ‘following more than two and a half years of implementation, around 150 deaths and around 400 hospital admissions, wholly attributable to alcohol consumption, were averted each year due to MUP,’ said PHS public health intelligence adviser Dr Grant Wyper. ‘The greatest reductions were seen for chronic alcohol health harms, in particular alcoholic liver disease, which were slightly offset with less certain evidence of increases in acute alcohol health harms. The findings highlight that the largest reductions were found for males, and for those living in the 40 per cent most deprived areas, groups which are known to experience disproportionally high levels of alcohol health harms in Scotland.’
Prof Sir Ian Gilmore: the evidence on this life-saving policy cannot be ignored any longer
The study painted a ‘very positive picture’ of MUP’s effectiveness, added Alcohol Health Alliance chair Professor Sir Ian Gilmore. ‘It strengthens the wealth of research already out there that shows MUP works to save lives, reduces pressure on the healthcare system and lessens the growing health inequality gap. The UK government must introduce this life-saving policy and bring us up to speed with our neighbours. The data and evidence are there, it cannot be ignored any longer.’
PHS is now bringing together the findings from a range of MUP studies for a report to be published in June.
Humankind’s Insight Enfield: Sort it! is set to launch in April 2023 providing free, friendly and confidential drug and alcohol support in the London Borough of Enfield for young people up to the age of 25, parents with drug or alcohol challenges, and families affected by a loved one’s substance use.
The service will be delivered by the national charity Humankind which supported over 90,000 people in 2021/22. Humankind delivers four young people’s services and three family support services across London as part of its Insight group of services. The Insight Services share a website, social media and good practice approach which the Enfield service will be part of.
Lyndsey Morris, Humankind Director of Operations for London and the South, said, “I am delighted that Enfield is joining the Insight family. We look forward to working with our local partners to provide free, flexible and judgement free support to local young people. Our services are focused on helping young people achieve their potential and be empowered to make healthy and safe decisions, that help them build a more resilient.
“Our family offer will support parents with drug or alcohol problems, families and friends impacted by substance use and children affected by their parent’s drug or alcohol use.”
The service has been commissioned by Enfield Council’s Public Health team and will launch on 1 April 2023 based at 29 Folkestone Road, N18 2ER. It will deliver support to young people and families from community locations across Enfield. To learn more please contact insightenfield@humankindcharity.org.uk or visit the Insight website.
This blog was originally published by Humankind. You can read the original post here.
DDN magazine is a free publication self-funded through advertising.
We are proud to work in partnership with many of the leading charities and treatment providers in the sector.
WDP has been shortlisted for the Best Healthcare Analytics Project for the NHS Award, Best Pharmaceutical Partnership with the NHS Award, and Most Impactful Project Addressing Health Inequalities Award at this year’s HSJ Partnership Awards, along with its partners in the Hepatitis C Drug Treatment Services (DTS) Provider Forum.
The HSJ Partnership Awards recognise the outstanding contributions made to healthcare across the UK and showcase these achievements on a national platform.
The Hepatitis C Drug Treatment Services (DTS) Provider Forum has been nominated for its ‘Hepatitis C Virus Screening in Drug Treatment Services’ initiative, which aims to eliminate Hepatitis C from UK drug and alcohol services by the end of 2023.
Membership of the Provider Forum includes a collection of the UK’s leading drug and alcohol service providers and The Hepatitis C Trust. The group’s members have been working together to implement a collaborative reporting and monitoring approach in Hepatitis C test and treat data.
The Hepatitis C Drug Treatment Services (DTS) Provider Forum is praised in the shortlisting for ‘Delivering National Improvements in HCV Screening for Individuals Accessing Drug Treatment Services’, and ‘Engaging the Disengaged in Drug Treatment Services through HCV testing and linkage to care’.
Marlon Freeman, Hep C Coordinator at WDP, said, “We are extremely grateful HSJ has selected The Hep C-Provider Forum to be a finalist in these categories. The hard work from its members is validated and shows appreciation in the mission to micro-eliminate Hep C in drug treatment services.”
There were at least 285 executions for drug offences worldwide in 2022, according to the latest report from Harm Reduction International (HRI). This represents a 118 per cent increase on 2021 and an 850 per cent increase since 2020.
There are 35 countries that still retain the death penalty.
Executions for drug offences were either confirmed or assumed to have been carried out in Iran, Saudi Arabia and Singapore, as well as in China, North Korea and Vietnam. Exact figures are not available for the latter three because of ‘extreme opacity’, says HRI, which means the numbers are likely to represent ‘only a percentage’ of the actual total. There were also more than 300 death sentences for drug offences imposed in 2022, a 28 per cent increase on the previous year, while more than 3,700 people were now on death row for drug offences worldwide.
However, there are also growing protests against the policy in many countries, HRI points out. ‘After defending its barbaric policy on the death penalty throughout 2021, Singapore issued execution warrants against individuals convicted of drug trafficking in February 2022,’ the charity states. A wave of protests followed, which are ‘rarely seen in the country due to extreme limitations on assemblies and the routine intimidation of activists’. There were also peaceful protests in Iran by families of people on death row, coinciding with a ‘surge’ of more than 250 confirmed executions, with many of the protesters arrested.
States and institutions, however, have ‘failed to adequately respond’ to the issue, HRI says, with UNODC failing to ‘take any public position on this practice for the second year in a row’. This lack of any political, economic or diplomatic sanctions for ‘blatant’ violations of international standards sends a ‘dangerous message to retentionist countries that executions, and therefore death sentences, can continue with impunity’ it states.
There are 35 countries in total still retaining the death penalty for drug offences, and known executions for drugs accounted for 30 per cent of all global executions, HRI points out. The figures, it says, are ‘a call to action to all actors involved in the fight for abolition, but primarily to governments and to intergovernmental actors: to acknowledge the barrier that punitive drug policies represent for the global fight towards abolition, and to identify and pursue new, influential strategies to promote the respect of international standards on the death penalty.’
Worldwide production of cocaine has ‘jumped dramatically’ in the last two years following an initial slowdown as a result of the COVID pandemic, according to the United Nations Office on Drugs and Crime (UNODC).
Coca cultivation increased by 35 per cent between 2020 and 2021, says UNODC’s Global report on cocaine 2023.
Coca bush cultivation is concentrated in the Americas, but there is strong potential for it to expand in Asia and Africa.
The increase is the result of an expansion in coca bush cultivation combined with improvements in the process of converting coca into cocaine hydrochloride, the document states, matched by a ‘swelling’ of demand. The rise in coca cultivation is the sharpest since 2016, it adds. While the cocaine market remains concentrated in the Americas and some parts of Europe, there is ‘strong potential’ for it to expand in Asia and Africa, and the report documents the emergence of new trafficking hubs in West and Central Africa, as well as South Eastern Europe.
The use of violence by criminal networks in Europe is also a ‘growing concern’ the report states, with a spike in serious incidents related to drug markets in recent years. These include ‘public shootings, bombings, kidnappings and torture’, and are partly the result of European cocaine markets attracting new trafficking organisations. According to some analysts, competition between criminal groups from the Balkans that has been driving targeted killings in Montenegro, Serbia, and Albania since around 2015 has now spilled over into other countries, the document says, with assassinations reported in Austria, Germany, Spain and elsewhere. Rivalry between multiple trafficking organisations in the Netherlands, meanwhile – including from Morocco – has led to a spate of assassinations and the discovery of shipping containers that had been converted into torture chambers
‘The surge in the global cocaine supply should put all of us on high alert,” said UNODC executive director Ghada Waly. ‘The potential for the cocaine market to expand in Africa and Asia is a dangerous reality. I urge governments and others to closely examine the report’s findings to determine how this transnational threat can be met with transnational responses based on awareness raising, prevention, and international and regional cooperation.’
Every Wednesday, nurses and recovery workers from Turning Point’s City & Hackney Recovery Service will be bringing high quality care straight to the most vulnerable in the community-with the new Clinical and Well-being van.
Rough sleepers are often most at risk from death at this time of year and beyond. Because many have mental health issues, no fixed address and chaotic behaviours, many services find that they are most ‘hard to reach’.
Rough sleepers will often fall between the cracks in over-stretched public services, and will become the most vulnerable to death and harm.
Reaching the ’hard to reach’
The City & Hackney Recovery Service, Hackney council, and partners are trying to address this problem through interventions and this new Clinical and Well-being Van. Originally bought by Public Health England for COVID testing, it has been repurposed, and is now fully equipped for those who would otherwise be at risk from health complications, and drug and alcohol issues.
Patients will be able to:
see a nurse for a full assessment of alcohol use to access detox and rehab services
get tested and treated for blood-borne viruses such as HIV and Hepatitis
have access to urine and blood pressure tests if needed
use a needle and syringe exchange and harm minimisation services
review and restart treatment to come off opioid drugs.
City & Hackney Recovery Service Well-being Nurse, Moore McClelland said, “We’ve started building up relationships with rough sleepers in the area – and we are reaching more. We have weekly meetings with professionals from other organisations to make sure our high-risk clients are being cared for.
“We’re also able to give out food vouchers, harm reduction medicine – such as Naloxone (to reduce death by overdose), and help signpost toward accommodation when the temperatures drop below freezing.
“Each week the clinical van will be targeting different places within City & Hackney to make sure we reach the ‘hard to reach’.”
A collaborative, cost-effective approach Jara Senar Villadeamigo, Strategic Manager (Hackney) added, “This project supports the team to work from a collaborative perspective. We rely on our relationships with the street and health outreach teams to know where we will have the greatest impact. This innovative approach will certainly inform how we develop the project in the future to meet the changing needs on the street.”
Recent studies show that interventions such as this, costs the public purse much less than letting the vulnerable in the community get to crisis point.
A recent report by charity CRISIS, calculated that the cost of a single homeless person for 12 months to public services is approximately £21,000 per year. This is versus the cost of intervention – which is approximately £1,500.
The City & Hackney Recovery Service Clinical and Well-being van is a cost effective intervention which will bring high quality care to people before they reach crisis point.
This blog was originally published by Turning Point. You can read the original post here.
DDN magazine is a free publication self-funded through advertising.
We are proud to work in partnership with many of the leading charities and treatment providers in the sector.
Scotland saw 295 suspected drug deaths recorded between October and December last year, according to the latest Police Scotland management information. The number is more than 25 per cent up on the previous quarter and the highest recorded in a single quarter since April to June 2021.
The deaths in Oct-Dec were 25 per cent up on the previous quarter
Overall, however, there were 1,092 suspected drug deaths recorded in the whole of 2022, which was 16 per cent down on the previous year. Men accounted for 70 per cent of the deaths, with deaths among women down by 9 per cent compared to 2021. As in previous years, two thirds of the deaths were in the 35-54 age group, with the Greater Glasgow police division recording the highest number of suspected deaths at 215.
The quarterly police figures are based on the reports of attending officers and are ‘not subject to the same level of validation and quality assurance’ as the annual official reports from National Records of Scotland, which are drawn from death certificates and pathologist reports.
Alex Cole-Hamilton: Accused Scottish government of taking its eye off the ball
In 2021 the country recorded its first fall in drug deaths in almost a decade, although it was by just one per cent. Scotland’s rate of drug-related deaths is three and half times greater than for the UK as a whole, and higher than anywhere in Europe. In its final report, the Scottish Drug Deaths Taskforce stated that the issue had not been given the priority it deserves (www.drinkanddrugsnews.com/time-for-a-complete-culture-change-says-drug-deaths-taskforces-final-report).
‘Every drug death is preventable, so I will never understand why the SNP, by its own admission, took its eye off the ball and chose to ignore the crisis as it unfolded,’ said leader of the Scottish Liberal Democrats Alex Cole-Hamilton. ‘As Nicola Sturgeon departs Bute House, she leaves behind an appalling legacy that is this country’s drug deaths crisis.’ Radical change was needed, he added, with his party calling for decriminalisation of drug use and implementation of consumption rooms.
Kirsten Horsburgh takes over as new leader of the SDF
Meanwhile, the Scottish Drugs Forum (SDF) has announced that Kirsten Horsburgh will be its new CEO from June this year, following the retirement of Dave Liddell. ‘I am delighted that Kirsten has been appointed as the next CEO,’ said Liddell. ‘Kirsten has worked with me for 11 years and since she started has shown excellent leadership qualities, initially in driving forward the implementation of the naloxone programme and latterly as director of operations. I look forward to working with Kirsten over the next couple of months to ensure a smooth transition into her new role.’
A new report from SDF states how Peer-to-peer naloxone programmes can help to reduce stigma and boost confidence, and if rolled out further could help to reduce Scotland’s drug-related death rate.
Suspected drug deaths in Scotland: October to December 2022 at www.gov.scot – read it here
Peer-to-peer naloxone programmes can help to reduce stigma and boost confidence, says a new report from the Scottish Drugs Forum (SDF), and if rolled out further could help to reduce Scotland’s drug-related death rate.
Peer to Peer naloxone training at the DDN Conference. This year’s event will be on 13 July in Birmingham
The document evaluates the impact of three pilot peer-to-peer programmes – one in an urban setting, one in a rural setting and one in a prison. SDF was involved in recruiting and delivering training, as well as interviewing the peers as part of the evaluation process. The peers were supported to train others and supply naloxone kits, ensuring that they had an ‘active voice’ in the sharing and promotion of good practice.
As well as increasing naloxone supply and training the programmes displayed other ‘tangible positive outcomes’, the report states. These included developing transferable skills, increasing confidence and employment opportunities, and reducing stigma towards peers from staff.
Among the document’s recommendations, however, are that peers should always receive proper payment for their work and that services should be fully prepared in advance in order to increase inclusion and set expectations. ‘All peer workers involved in projects of this kind, including those within prison settings, must be paid fairly for their time,’ the report states. ‘This will allow the role to be recognised as important work and ensure peers are valued.’ Staff also need to be aware of how sessional or part-time employment can affect peers’ benefits, adding that ‘when peers apply and become involved with this work, clear expectations about the role and its parameters and related processes must be explained to them, such as the need for ID and how long PVG/background checks may take.’
‘With sufficient staff time and resource, including payment for peers, and awareness of logistical and practical challenges, there are no reasons why this approach could not be continued in these areas and rolled out in others effectively,’ says SDF. ‘There should be a confident assumption that this would contribute even further to the reduction of drug-related deaths in Scotland due to increased naloxone supply and broader efforts for peer inclusion.’
‘This report clearly shows the power of peer involvement, not only on increasing distribution of naloxone and saving lives, but on changing attitudes and approaches to work in the field,’ said research and peer engagement senior officer at SDF Samantha Stewart. ‘The evaluation demonstrates that including peers and treating and paying them equally should be a non-negotiable in this and other types of work across the service landscape.’
Peer naloxone supply project: an evaluation of three pilot areas available at sdf.org.uk
See the May issue of DDN for an interview with outgoing SDF chief executive David Liddell
Humankind has signed a joint letter to the the Chancellor of the Exchequer calling to reinstate funding to support children affected by parental alcohol use.
The Chancellor of the Exchequer, Jeremy Hunt MP, will deliver his Spring Budget in Parliament on Wednesday 15 March.
Through the Alcohol and Families Alliance, of which Humankind is a member, Humankind signed a joint letter to the Chancellor at the beginning of March calling for him to reinstate funding to support children of alcohol dependent parents.
The Alcohol and Families Alliance is a collaboration of over 40 organisations that is united in reducing the harms experienced by families through alcohol.
Established in 2018, the Children of Alcohol Dependent Parents grant enabled ground-breaking work to take place, benefitting many children of alcohol dependent parents by allowing them and their parents to turn their lives around.
Reinstating this grant will provide children affected by parental alcohol use with access to the support they need and ensure that they are not forgotten, or neglected, but empowered to enjoy healthy and secure childhoods.
Alongside last month’s welcome confirmation of treatment funding until 2025, the government also announced more than £50m to provide targeted housing support for people in treatment and recovery – the first time this has happened as part of a national drug strategy.
DDN hears from OHID’s Rosanna O’Connor about the grant’s aims and ambitions.
Last month saw the sector breathe a collective sigh of relief when the government confirmed its allocation of treatment funding for the next two years – more than £154m for 2023-24, followed by indicative funding of almost £267m for 2024-25. The announcement provided certainty and allowed the field to properly plan for the future, said Turning Point’s chief operating officer Clare Taylor, one of many leading figures in the sector to publicly welcome it (www.drinkanddrugsnews.com/government-confirms-421m-treatment-funding-for-next-two-years).
Priorities
The new funding would prioritise the areas with the greatest need, the government said, and enhance both treatment capacity and quality. As well as providing more residential rehab and inpatient detox places, it will also address the sector’s staffing crisis. All of this is, of course, sorely needed. But last month also saw a separate announcement of up to £53m to improve housing support for people in treatment and recovery.
According to the latest OHID figures, a sixth of all people entering treatment – and a third of those entering treatment for opiates – reported having a housing problem, and according to Crisis two thirds of people experiencing homelessness cite substance use as a reason for becoming homeless in the first place.
Housing first
Rosanna O’Connor, director of addictions and inclusion at the Office for Health Improvement and Disparities
Everyone now agrees that good quality, stable and affordable housing is a crucial part of ensuring successful recovery, but is it something that’s perhaps been overlooked in the past? ‘Although the importance of housing in supporting recovery has been emphasised in previous national drug strategies, this is the first strategy where funding has been secured to help us understand what works,’ Rosanna O’Connor, director of addictions and inclusion at the Office for Health Improvement and Disparities (OHID), tells DDN.
The funding will be allocated to 28 local authorities across England with the greatest need, and as well as allowing local areas to set up schemes tailored to their local populations it will also be monitored to help develop an evidence base.
Among the approaches chosen are specialist housing caseworkers operating from prevention hubs in Manchester, people with lived experience helping those struggling to maintain independent living in Wigan, and cross-department training to create joined-up care for people experiencing homelessness in Lancashire. Why was this chosen?
‘OHID worked closely with the Department for Levelling Up, Housing and Communities to design a menu of housing support interventions that we thought could have the greatest impact on the housing needs of people in treatment and recovery,’ says O’Connor. Eligible local authorities were then asked to submit funding plans based on this, but with the flexibility to propose their own interventions.
‘The main categories for the menu were specialist substance misuse floating support workers and housing specialist caseworkers,’ she says. ‘Areas have submitted plans that include a range of different posts within these categories, some focusing on specific populations accessing treatment with housing-related needs, such as women or people leaving the justice system.’
Community approach
Manchester’s approach is being supported because ‘we know how important it is to get support workers into the community, rather than waiting for people to be referred into their services’, she states. ‘That’s why providing floating support into a range of accommodation settings is a core part of the housing support grant. We’re funding interventions based on the need in local areas – for example in Middlesbrough, a team of specialist caseworkers will carry out homelessness assessments and provide continuity of care to people leaving prison.’ Hertfordshire, Manchester and Bristol are also considering similar roles, she says.
Recruitment and retention of the workforce is clearly a key challenge, she points out, and local authorities are being encouraged to fund training and support through the grant to ensure their staff have the knowledge and skills they need.
‘We know that integrated or multi-disciplinary teams, such as the one we’re funding in Lancashire, can provide a better offer to people through a more joined-up approach – and encouraging staff to learn from each other and network through training opportunities is a key part of that. Oxfordshire is introducing a new health and housing coordination role to deliver a programme of training across housing and drug and alcohol services, while in Bradford a training and development co-ordinator will develop and coordinate a training academy and source training, development and learning for staff working on the housing support grant.’
The programme will also be funding specialist support for people with an acquired brain injury that has been caused or exacerbated through alcohol or substance use.
Affordability
However ambitious and well-intentioned this all is, however, there’s a long-standing and acute shortage of affordable housing in the UK – how much of a challenge is this going to be in terms of properly addressing the housing needs of people in recovery?
‘This is obviously a challenge that goes beyond the scope of the drug strategy housing support grant to solve,’ she says. ‘But the grant has been set up so we can test and learn how to approach providing this type of support, and we have purposefully ensured regional representation so that we can also test the impact of these variations across the regions.’ DDN
WDP and The Nelson Trust are teaming up to open a specialist women-only detox centre – the only one of its kind currently in the UK.
Photo by Becca Tapert on Unsplash
While there are some women-only residential rehabilitation services available, there is currently no women-only inpatient detoxification service in the UK.
A lack of women-only detox provision is a major gap and specific barrier to residential rehabilitation, as detoxification is often required before women who are dependent on alcohol or drugs can access rehab.
WDP and The Nelson Trust will be drawing on their respective and complementary strengths to open their women-only inpatient detox in Gloucestershire later in the year, ensuring that lived experience is front and centre of the design and development.
Anna Whitton, CEO at WDP, said, “We are delighted to be collaborating with The Nelson Trust to find a solution and address this worrying gap in women’s treatment provision in the UK. Our significant experience, expert knowledge and clinical excellence in inpatient detoxification will help us provide bespoke, safe and supportive care for vulnerable women with complex needs at our new centre.”
John Trolan, CEO at The Nelson Trust, added, “Having worked with WDP over many years now we’re really excited and looking forward to further developing a collaboration around trauma-informed women specific detox.”
If you would like to support or get involved with the development of this new initiative, please contact Anna Whitton on anna.whitton@wdp.org.uk.
This post was originally published by WDP. Read it here.
DDN magazine is a free publication self-funded through advertising.
We are proud to work in partnership with many of the leading charities and treatment providers in the sector.
The government has announced a £5m innovation fund to trial new ways of reducing what it calls ‘so-called recreational drug use’.
The fund includes provision for education events and pop-up pods at festivals.
Five projects have been allocated £734,000, with the remaining money to be made available in two further phases.
The projects included in phase one of the fund are located in Derbyshire, Dorset, Huddersfield, Manchester and the South East of England and are tailored to meet local needs, the Department of Health and Social Care (DHSC) states. These include education events and pop-up pods at festivals, training for door staff and workforce support to reduce young people’s vulnerability to drug use.
Each of the projects will receive initial funding to help them develop their interventions for later evaluation. The successful projects will then be able to apply for further funding in phase 2, as will other new projects, while those that show positive results after evaluation and implementation will be considered for national roll-out.
The selection process for the projects focused on encouraging creativity and innovation in finding ways to prevent people going on to problematic or dependent use in the future, DHSC says. ‘Projects like these will pave the way for new research into preventing drug addiction and enable us to meet our national strategy aim to cut drugs and crime,’ said health minister Neil O’Brien.
One successful project is the Derbyshire-based 1625 Outreach service, which is run by Change Grow Live in partnership with Middlesex University and focuses on early interventions to reduce demand and harm.
Zoë Welch, Head of Research at Change Grow Live.
‘The innovative multi-strand approach works across rural and urban settings in Derbyshire and Derby city offering education programmes, responsive outreach, a branded van and pop-up pod at festivals/events, digital interventions, and night-time economy staff training,’ said head of research at Change Grow Live, Zoë Welch. ‘Our aim is to prepare 1625 Outreach for robust evaluation through literature review, stakeholder feedback, data linkage and creative methods to capture process and outcomes. We will use desk research, PPI, stakeholder consultation, and county-wide collaboration to refine the model and develop a framework to evaluate the different strands of outreach activity.’
The current evidence suggests that the harms associated with nitrous oxide (‘laughing gas’) are ‘not commensurate with control under the Misuse of Drugs Act 1971’, the ACMD has said in its updated assessment of the drug. The types of harms caused by nitrous oxide have not changed since the ACMD’s last report it 2015, it adds.
The report recommends that nitrous oxide remains under the Psychoactive Substances Act 2016, but that additional measures are needed to raise awareness of the risks associated with use and tackle non-legitimate supply. Banning the drug, however, would place ‘disproportionate burdens’ on its legitimate use in medical, industrial and commercial fields, the report says. Then-secretary Priti Patel said when the review was commissioned that the Home Office stood ‘ready to take tough action’ if the ACMD recommended a ban.
Priti Patel was ready to take tough action
While the number of deaths and demand for treatment for problematic use are low compared to other drugs, there have been reports of increasing levels of neurological harms – including nerve and spinal cord damage – associated with heavy use. This is particularly an issue with larger-volume cannisters, the report adds, and there have also been anecdotal reports of people driving under the influence.
It is ‘clear that additional measures are needed’ to reduce the health and social harms associated with nitrous oxide, the report states, and goes on to make seven recommendations. These include restrictions on cannister sizes that don’t have legitimate uses and on direct-to-consumer sales, increased health warnings, and shutting down websites involved in non-legitimate sales. It also recommends more information and advice being made available via healthcare staff and at festivals, as well as better monitoring of health and social harms.
ACMD chair, Prof Owen Bowden-Jones: the report gives recommendations to limit harm
‘Nitrous oxide remains a widely used drug in the UK,’ said ACMD chair Professor Owen Bowden-Jones. ‘While the number of deaths related to nitrous oxide remains low compared to other drugs, there is evidence of increasing neurological harms in people who use nitrous oxide in a persistent and heavy way and also reports of increasing social harms such as littering of canisters and driving under the influence. Today the ACMD has made a number of recommendations to tackle these emerging harms including restricting availability, giving local authorities and police proportionate powers to intervene, and educating people who use nitrous oxide of the harms and how to reduce them. Tackling any type of drug use requires careful consideration of not just the drug, but the broader circumstances in which drug use takes place. No one intervention will succeed alone, but taken together, we believe that these measures will help to reverse the recent increase in harms, for the benefit of all.’
Nitrous oxide: updated harms assessment – read it here
Following the Drugs, Alcohol and Justice APPG’s look at the challenges for women accessing treatment in last month’s DDN, Anna Whitton describes some developments at WDP and across the sector when it comes to improving women’s treatment provision.
The Collective Voice ‘Women’s Treatment Working Group’ launched on International Women’s Day 2021. Comprised of female leaders who come together to make a difference, we share practice, influence our respective organisations, and advocate externally on the need for improved drug and alcohol services for women.
Central to our approach is a recognition that there are much-needed changes that we can take responsibility for. There are of course also many areas where we need to harness our collective influencing power, including how we might influence systems and policy change to drive improvements for women. Our presentation to the Drugs, Alcohol and Justice All-Party Parliamentary Group last month (DDN, February, p23) is an example of this work. To find out more about the group, check out our page on the Collective Voice website at www.collectivevoice.org.uk/womens-alcohol-and-drug-treatment.
This collaborative approach is especially timely – women have been under-represented in services for too long, and the data presents a worrying picture. Drug-related deaths among women have been increasing for more than ten successive years – for example there were 195 cocaine deaths in 2021 compared to 19 in 2010.
Learning from research, sharing practice through the Women’s Treatment Working Group and hearing what the women who come to our services tell us, we have been reviewing and refreshing how we do things.
As part of a broader trauma-informed approach with women-specific interventions, practical steps are being strengthened across all of our services, such as:
Implementing women-only spaces – spaces and times of day where men (staff and service users) are not present.
Setting up accessible appointment times – for example, making sure that women who are the sole/main person responsible for childcare do not have appointments scheduled during half-terms, and not offering appointments outside of school or nursery hours or too close to pick-up/drop-off times.
Offering alternative appointment venues – looking at other options in the community which might be easier to travel to – such as somewhere they already have other appointments at – or a place they feel more comfortable meeting in.
Arranging for female workers to attend probation on a Friday – as this is often when people are released from prison, ensuring that there are female workers available for any women who need to meet with their local treatment service on the same day.
Connecting with family support providers – for example, we are building relationships with Home Start in our local areas.
Working closely with specialist women’s centres – enabling access to treatment through safe women-only spaces where women can also access a wider range of support to meet their needs.
We are also excited to be launching a women’s co-production audit across our services. We think it’s important to make sure that that we really hear women’s voices and work together to implement change – our new audit will help us to do that. Together, we will be assessing what we currently have in place and, from this month onwards, we will regularly audit our services with women to establish what we are doing well and what we could be doing better.
As well as looking at areas of improvement and best practice, the Women’s Treatment Working Group shares learning about what is currently available nationally and where there are gaps in treatment provision.
At WDP, we had been talking with The Nelson Trust about women’s treatment needs, as they have a strong track record in delivering women’s services including women-only residential services. They had already identified a lack of women-only detox provision as a major gap and specific barrier to residential rehabilitation, as detoxification is often required before women can access these services.
While there are some women-only residential rehabilitation services and more in development – for example, Phoenix Futures and Ley Community are opening a site in Oxfordshire later this year – there is currently no women-only specialist inpatient detoxification service in the UK.
Anna Whitton is CEO of WDP
Together with The Nelson Trust, we were committed to finding a solution and are now addressing this gap by implementing a women-only inpatient detoxification. This collaboration draws on the respective and complementary strengths of our organisations, incorporates lived experience in co-design and development, and will involve the mobilisation of a new site in Gloucestershire, which we anticipate will open this year.
As part of this exciting provision, we will be recruiting for some new and interesting women-specific roles so keep an eye out. If you’d like to support or get involved with the development of this new initiative, please contact me on anna.whitton@wdp.org.uk.
Women supporting women – stories from the frontline
Online Event 8 March, 10 – 11.30
What is good practice when working with women in drug and alcohol treatment services?
Are you working with women with drug or alcohol issues?
Do you want to better understand what gender responsive treatment looks like in practice?
Do you want to hear ideas to improve outcomes for women?
Join Collective Voice on International Women’s Day, Wednesday 8 March, between 10 and 11:30am to explore good practice when working with women in drug and alcohol treatment services. The webinar will be chaired by Phoenix Futures chief executive Karen Biggs and will feature a range of speakers from frontline service delivery alongside lived experience testimony:
Working with women’s trauma: practical tips and hints to help build your toolkit when working with traumatised women (Evgenia Stefanopoulou, Turning Point)
Voices of lived experience: themes and reflections from women using services (April, Working with Everyone)
Meeting women where they are at: examples from practice of creative ways to engage with women – from drop-ins to menopause support (speaker tbc)
There will be a Q&A after the presentations, so please do join us to share your thoughts on this crucial topic.
An effective workforce needs high quality training.We need to look at staff training urgently if we’re going to tackle a skills deficit fuelled by underinvestment and lockdown, says Kevin Flemen.
This is my twentieth year working fulltime as an independent trainer in the drug sector. Two decades of flipcharts, the odour of marker pens and the slow shift of technology from OHPs, through projectors to Plasma TVs and Zoom training. In that time I’ve gone from the full-scale training lunch menu in hotels to half a packet of biscuits in a training room with no working heating!
I’ve survived austerity, COVID lockdowns and more Home Office drugs ministers and drug strategies than I care to remember. I dread to think how many trees’ worth of flipcharts I’ve gone through or how much coffee I’ve drunk. I’ve also never been busier. People looking to book training now are crestfallen when I say that I’ll probably be booking them in for March…2024.
Experience deficit
While it’s good to be busy, it’s not ideal. As a sector the gap between training need and halfway decent trainers to deliver it has never been greater. This has serious implications for any expansion of services or enhanced delivery. The days when there were so many trainers out there that they had their own supplement in DDN are long gone.
The need has grown in part due to COVID. The sector, which had been losing workers rapidly anyway, lost still more during lockdown, and so many of these were older experienced workers who took with them years of knowledge. Posts were frozen and then as lockdown continued, recruitment resumed. But as numerous services will attest, it’s not always easy to recruit staff, especially those with experience and especially outside urban areas. I’ve had so many people on courses who are recent graduates, have changed careers or have limited experience in a related sector.
These workers in a normal working environment would learn on the job – shadowing, team meetings, supervision, training sessions and conversations with colleagues in the kitchen. But being recruited in lockdown, they had no chance to do these things. There might be some reading material, videos online and dialling into meetings on Teams. Some did lots of their own background reading, looked things up and did their best to figure it out. But in short-staffed services with high caseloads, these new workers were needed quickly and so were seeing clients. In lockdown this was likely to mean seeing people online, with no chance to shadow or nip to ask a colleague’s advice.
Complex cases
No surprise then that some of these workers left within months. They hadn’t been recruited with the required skills and weren’t properly trained. Given complex cases with limited training and support they felt under-skilled, unsupported and anxious about doing the wrong thing. The relief of those attending live training sessions (whether online or face-to-face) was palpable.
Trainers too have had to learn and adapt. Whether it’s getting to grips with online training platforms, investing in new equipment, or getting back to training in the real world against a backdrop of strike chaos, it’s neither easy nor straightforward. Economic downturns and COVID meant that a fair few freelancers couldn’t adapt their offering and dropped out.
I’ve been relatively lucky. There’s a cohort of purchasers with whom I have worked for a number of years, whose support during lockdown was invaluable. It was mutually beneficial – we kept each other going through lockdown and we’re still there for each other on the other side. Now however, there are lots of people getting in touch, desperate for training with unspent budgets to spend and desperately looking for trainers with capacity.
Training matters
Training matters so much to organisations – now probably more than ever. It’s a shame that for too many organisations it’s been relegated to a video, an online pack or being directed to some TED talks. The people you recruited deserve better and the people that you provide services to need more.
Sooner rather than later
Earlier purchasing of training is more likely achieve successful outcomes and a more organised process.
1.Ask around about trainers.
They’re not all the same and availability does not equal quality. It’s a false economy to run bad training – it takes staff away from their roles and you need to repeat the training later on. Buy good training first time.
2. Ensure your staff know you are valuing them by getting good training.
And invest in the event. A cluttered messy room, knackered projector, no biscuits and a lack of flipchart says you don’t care about the training – so why should participants?
3. It’s not face-to-face or online
It’s a mix of both, and hybrid courses where required. Some courses run best face-to-face (such as safer injecting courses) and others can happily run online (like our drugs and the law course).
4. Plan for the next two years NOW
Yes, I know you need your staff trained next month but we should have started this conversation last year. Develop a training programme across the team, discuss it with your trainer(s) and schedule it now for this year and next year. Then you know you have the dates you will need.
5Use a balance of in-house and external training
For all your internal processes and induction-related training, in-house courses are the best. But be careful of using in-house courses for everything. External trainers are the butterflies of the sector. We flit from service to service, learning about what’s going on and cross-pollinating ideas. And that external perspective can add huge value – we can see the gaps you’ve stopped seeing.
6.You shouldn’t just be getting the training
It’s the discussion before, the engagement with participants during and after the course, the resources and all the other elements that give the session life beyond the six hours of the actual session.
7.Whenever you can, get training to take place off-site.
When training takes place in the project group workroom, staff inevitably get drawn back to their desks at lunchtime or pulled away to take calls or see clients. This detracts from their ability to immerse themselves in training.
8. There are some good trainers and some mediocre ones
There are also a few that shouldn’t be allowed near a flipchart. Find the good ones. Build a relationship. Don’t treat them just as hired help. They will get to know your organisation, your staff and your issues. They can help you with these issues more than you realise. And the good trainers can choose who they work with.
9. Invest in your future trainers now!
Few posts have a training component built in. It’s a useful tool in its own right. Training is communication and it helps workers in group work, in presenting to colleagues and partner organisations, and in their career development. Take the workers with a passion for their jobs. Enhance their training skills. And they will become the next generation of amazing trainers to maintain skills in the sector for the next 20 years.
Kevin Flemen runs the drugs training service KFx (www.kfx.org.uk). He’s booked up a fair way into the future but you can email him at kevin@kfx.org.uk. He occasionally tweets @kfx news.
A new framework of actions for prescription medicines has been published by NHS England, in partnership with leads and representatives from local integrated care systems (ICBs).
Professionals should regularly discuss prescriptions with patients
The actions set out in Optimising personalised care for adults prescribed medicines associated with dependence or withdrawal symptoms have been co-produced with patients, lived experience groups, charities and national bodies like NICE, NHS England states.
The framework focuses on five key actions – personalised care and shared decision making, alternative interventions, service specification and change management, taking whole-system approaches, and population health management.
Professionals should regularly discuss prescriptions with patients, the framework states, including the potential benefits and risks and whether to stop or taper the treatment, with these reviews used to offer alternatives where appropriate. Services for people experiencing withdrawal symptoms and alternative treatments should also be built into service specifications, it adds.
Local support services for people experiencing dependence problems was a key recommendation of PHE’s Prescribed medicines review in 2019. The review studied dependence and withdrawal issues associated with five commonly prescribed classes of medication – opioids for pain, benzodiazepines, ‘z’ drugs like zopiclone, antidepressants and gabapentinoids. It found that one in four adults had been prescribed at least one of these during the previous year, with half having been prescribed them for a year and a third for three years or more (www.drinkanddrugsnews.com/prescription-drug-addiction-phe-review). This is despite benzodiazepines, for example, not being recommended for use lasting more than a month.
The review also found wide variations in prescribing rates, with prescribing levels and prescription lengths for opioids and gabapentinoids both higher in some of the country’s most deprived areas. It also highlighted harmful withdrawal effects lasting months or years, and lack of support services for people experiencing problems.
Ex NHS CEO, Lord Crisp
‘For decades, patients have experienced often life-changing withdrawal symptoms from medicines such as sleeping pills and antidepressants with almost no support or recognition from the health service,’ said co-chair of the APPG for Prescribed Drug Dependence and ex NHS CEO, Lord Crisp. ‘The APPG for Prescribed Drug Dependence welcomes this new framework for action from NHS England, which should lead to the delivery of services across the country to help those who are suffering. However it will take months or perhaps years for these services to be developed.
In the meantime we call on the government to implement its own recommendation for a 24-hour national helpline and website to support those in crisis today. Together these initiatives will save lives, reduce suffering and bring down the unnecessary costs to the public purse.’
Needs-led, wraparound services are vital to tackling homelessness, says Vanessa Johnson.
Homelessness is a growing scourge in British society, which the government seems unable – or unwilling – to tackle. People find themselves homeless for a variety of reasons, including mental health challenges, loss of income, and/or substance use.
While many people’s ideas of homelessness are based on street homelessness, this is just the tip of the iceberg. According to Shelter, homelessness applies to anyone without a permanent home – the ‘hidden homeless’ includes those living in unsuitable or temporary accommodation, in hostels or bed and breakfasts, those temporarily staying with others, or those who are sofa-surfing.
Social Interest Group (SIG), as a group of charities, offers a range of integrated support services with an emphasis on prevention, early intervention, integration, and recovery for people at risk of losing – or who have lost – their independence.
We offer support services, interventions, and opportunities through:
Supported accommodation – either temporary or longer-stay projects for up to two years, with onsite staff support to recover from a period of instability, to prepare for independent living, and to offer a safe and secure home to those who need additional support while focusing on resident asset building and becoming active citizens.
Housing-related floating support – a peripatetic service offering needs-based individualised support to enable residents to live independently and successfully in their own communities.
Community-based recovery services – creating community-based opportunities for residents, members, and volunteers to engage in social, learning and therapeutic activities and groups to develop skills and reintegrate into their communities.
Hidden Homeless
I spoke with Emmeline Irvine, our head of services and specialist lead for homelessness and complex needs. She explained how homelessness is tackled across Luton, where she’s based. ‘Like many of us working across SIG, homelessness is an issue and challenge that is never far from our thoughts at every level – from frontline work to partnership working and our trauma-informed approach to policy and best practice development,’ she says.
‘One of my primary locations of concern is Luton, where many of our services are located. More than 3,450 people are homeless in Luton – one in 66 people. Luton has seen a slight decrease in the number of rough sleepers, but our experience suggests that homelessness is becoming more hidden. The cost-of-living crisis and the lack of affordable housing is only going to further impact the number of people needing support to be accommodated safely in appropriate housing with the right support.’
It is vital to offer needs-led, wraparound support to meet the needs of those experiencing homelessness, she stresses, and Housing First is a familiar model to most – ‘whereby safe and secure accommodation is provided, with no conditions of tenancy, offering people who have experienced homelessness and chronic health issues and have social care needs a stable home from which to rebuild their lives.’
Locally, SIG Penrose is part of the Bedford Homeless Partnership and the Luton Homeless Partnership, and the value of these partnerships is vast, she says. ‘They can help to challenge myths and stigma around homelessness and provide opportunities for like-minded organisations to work together, along with local authorities, to gather data and insight and find solutions.’
Understanding trauma is also key. ‘Having a trauma-informed approach is essential, as positive change for people who have experienced homelessness can be a long journey. The links between homelessness and isolation, unemployment, poverty, and mental ill health are well documented and require a truly holistic approach.
Building Trust
‘In Luton, we’ve been looking at the challenge of people not accepting accommodation where offered – we need to work as a partnership to understand the various reasons why the offer of somewhere to live may not be enough to break the cycle of homelessness for some. In December 2022, the Luton rough sleeping teams were aware of 25 people who were rough sleeping, but five of those did have accommodation available to them. For those of us working in temporary accommodation and homelessness provisions, we understand that building trust is key to positive engagement. So we work alongside our homelessness partners in Luton to offer an approach that covers housing, mental health support, substance and alcohol support, and primary care needs, and we take the offer to the street homeless population to make those initial links.’
Continued presence
SIG will continue to play its part in supporting people experiencing homelessness. Our services and geographical locations work to deliver homelessness services, especially in Kent, through our Pathways to Independence services, and in the Royal Borough of Kensington and Chelsea through the SIG Penrose Complex Needs Hub. We have a wealth of knowledge and a broad range of services across the group, and we work together to shape best practice. But one thing is certain – homelessness should not become the norm for those who find themselves in difficulties.
Vanessa Johnson is communications manager at SIG.
From the street
As a charity, SIG sees the effects of homelessness firsthand and increasingly supports people experiencing homelessness in some of its services. Two residents share their experiences.
Soren’s Story
Soren did a variety of jobs in his 20s, usually losing them as a result of his drinking. At 27, his GP referred him to Ealing RISE and he went into detox. Offered a flat by the local council, he was abstinent for around nine months before again losing his job. After a two-week spell in prison he ‘spiralled out of control’, eventually losing his flat. He was offered another detox place but couldn’t accept it as he was homeless. He was then accepted at a ‘wet house’, where he relapsed again.
He was now street homeless, but after attending a series of 12-step programmes he entered Cherington House in Ealing. He’s been there for 18 months and has been sober for around two years. He still attends RISE and goes to AA meetings but believes there’s a lack of understanding around the links between homelessness and factors like substance misuse.
‘For the majority, there’s not enough help,’ he says. ‘People must want to change and need gentle support, not preaching and ultimatums. People that look down on the homeless don’t realise they can only be one or two pay cheques away from being there too.’ He hopes to move on to independent living, but only when the time is right. ‘I will need extra support, though. I know what it takes to stay sober, but I’m learning what it takes to live sober. Because staying sober and living sober is different. That’s where the hard work and aftercare come in.’
Wesley’s Story
Wesley* first became homeless early in 2022, but was not street homeless for very long. He’d been arrested the previous year and charged with bodily harm and criminal damage (to his own property). Although the assault charges were dropped, he went from living with his partner and children to moving back in with his parents. He’d been drinking heavily since 2017, eventually losing his job. ‘Alcohol’s sole intention is to isolate you from everyone so it can control you,’ he says.
After falling out with his parents he went to the Medway Council’s offices and told them that he needed help, and was eventually referred to SIG Pathways to Independence. He now lives in a shared house, and is hoping to be permanently housed. He volunteers, and is in touch with Turning Point and Open Road. He’s also started adult education classes, and has contact with his children and extended family.
‘When you find yourself alone even though there are others around you, with nowhere to go, that’s what rock bottom means to me,’ he says. ‘I’m grateful that I’m in contact with my family again. It took a lot of hard work to build trust again but it’s the fear factor of knowing that I have a lot to lose that keeps me going. I’m tremendously grateful to Pathways. I’m living just for today. I have to make the right choice. My message to anyone who finds themselves in similar circumstances is to ask for help.’
Soaring rents, stagnant rates of housing benefit, and many more families facing homelessness. The investments in the drug strategy and rough sleeping strategy are a vital intervention but we need to heed Crisis’ call for a more preventative homelessness system (p15). There’s a key role for drug and alcohol workers here in making the integrated care systems a reality, right from the commissioning stage, so in this issue we’ve had a look at some of the excellent work going on around the country to address homelessness and the many complexities that relate to it.
It’s all about having a safe space, and not just a roof over your head. And that’s where all those different elements of support are so important, whether they offer a refuge from abusive relationships, a chance to break with a compulsive behaviour such as gambling, or a chance to detox or stabilise.
These are, of course, demanding roles – and you need to be confident as well as qualified to work well with such diverse tasks and specific issues that have a direct bearing on someone’s health and wellbeing. It’s not the situation to take a guess. So here’s an interesting question: has your training and professional development suffered at all since the pandemic (p16-17)? Have a read and let us know because we’re looking at careers in our next issue. Are you getting the support you need?
There are set principles that anyone working with people with complex needs should adhere to, say Dr Stephen Donaldson, Ben Sweeting, Richard Croall and Edward Loveless.
Multiple disadvantage is a term used to describe people who have experienced or are experiencing multiple difficulties, including repeat street homelessness, trauma, substance misuse, physical health difficulties and mental health problems. These challenges often – and understandably – impact on people’s engagement with services, psychological wellbeing, physical safety, and sense of connection with society. People faced with these challenges regularly fall between the gaps of services and, over time, hope and trust in others can be lost. This can lead to people feeling trapped in a cycle of wanting help, not asking for help or asking in ways that communicate their distress through behaviours which are harder for some to understand.
The REACH (Reducing Exclusion for Adults with Complex Housing Needs) team was set up to work with those who are street homeless and experiencing mental health difficulties and substance misuse in Scarborough and Whitby.
The team takes a partnership approach with multiple service partners coming together to support the person in their journey of recovery. Our vision is to support people to have housing stability, through a Housing First model. But while having a home is important, it’s only the tip of the iceberg. Given the multiple disadvantages experienced, working with people to help them manage addiction, trauma, and their mental health difficulties is key to stability and change. Everyone deserves to have a life worth living, but this can be a long and bumpy road to travel.
As part of our developing work in the area, we’ve been reflecting on some of the shared principles we hold to guide what we do, with the hope of developing practice-based evidence in this area.
PRINCIPLES OF WORKING
We developed a set of guiding principles to support the interventions and work we do.
MEET THE PERSON WHERE THEY ARE AT
This principle, given the repeat homelessness experienced by this client group, is both physical – in terms of being present with people on the street – and psychological, in terms of acknowledging that traditional approaches to assessment, formulation, safety planning, care planning and intervention all need adapting to support the person. It’s also important to think about the reality of the person’s position and ensure that goals and expectations around engagement are realistic and don’t set people up to fail, preventing a further cycle of service disconnection, abandonment, and perceived failure.
RELATIONAL CONNECTION AT EVERY OPPORTUNITY
As past trauma is a significant contributor to substance misuse and mental health issues, it’s essential that every contact takes a relational-trauma informed stance. Each contact has the potential to harm or heal, and therefore the primary focus is on building a psychologically safe frame within which therapeutic attachment and intervention can take place. This ensures that the people we work with can feel emotionally and psychologically safe.
FORMULATE THE PERSON AND THEIR RESOURCES
Often people are referred to our service with a collection of labels, diagnoses and narratives, and what can get lost is the person’s story and experiences. Within our model, hearing the person’s narrative of their experiences and resourcefulness, alongside their challenges, is significant. Having a co-created, shared narrative helps the person feel heard, while also ensuring that an understanding of what has happened to them – and how we may be able to help – is realistic and transparent.
BE CREATIVE, FLEXIBLE, AND CONSISTENT
To work with people who have experienced substance misuse, mental health, loss and trauma requires a great deal of creativity and flexibility. This can mean a significant adaptation of how we’ve traditionally gone about engaging with people. However, it’s equally important that there is consistency, boundaries and clarity in the approach. Often people have felt let down and abandoned, so consistency in engagement is paramount to rebuilding a sense of trust, while boundaries offer a sense of physical and psychological safety. This process is not without its challenges, with ruptures and repairs within the therapeutic relationship being a common and often necessary part of the trust building process. For clinicians, openness, curiosity and not enacting rejecting or rescuing behaviour is key.
ADVOCATE FOR THE PERSON IN THE SYSTEM
Organisational systems and processes are complex and can, for many service users, feel difficult to negotiate. It’s therefore key that we advocate alongside the person to help them access what they need. However, it’s very common for people to be seen as hard to help as a result of stigma and harmful narratives. These narratives and experiences of rejection have often exacerbated a sense of disconnection from society and loss of hope for many of those we work with. Advocating for the person is important in supporting change, but there’s also a significant role in supporting the wider system to challenge its own views, narratives, and ideas about people and the ways they present.
MAINTAIN OPTIMISM AND HOPE – DON’T GIVE UP
Given the multifaceted nature of the difficulties and challenges the people we work with face and present with, it can feel clinically overwhelming at times. A cyclical process of change-stability-lapse-relapse-change is the norm. For many professionals this process can challenge the fundamental values of why we work in this field, our own sense of clinical competence and at times lead to a perception of not being good enough at our jobs. For this client group this can be experienced as rejection – where they’re seen as too complex and passed to someone else or told they need something else, further exacerbating a sense of hopelessness. Having access to regular, consistent and skilled psychological supervision is therefore a must-have.
This approach of a psychologically informed frame is not easy, and can face constant challenges. However, it’s ultimately the only way to consistently support stability and recovery for those with complex homelessness, substance misuse and mental health needs. By ensuring this frame and its principles are in place and constantly reflected on maintains clinical optimism, shared understanding, and collaborative partnership working. Overall, this approach ensures that the care provided is stabilising rather than inadvertently damaging, thus working to reduce further trauma and enhance the quality of life of those in need.
Dr Stephen Donaldson, Ben Sweeting, Richard Croall and Edward Loveless.
Dr Stephen Donaldson is consultant clinical psychologist, Ben Sweeting is advance nurse practitioner, mental health, and Richard Croall is advance nurse practitioner, dual diagnosis – all at the REACH team. Edward Loveless is assistant psychologist, Tees, Esk and Wear Valley’s NHS Foundation Trust.
WDP has been successful in its bid to deliver a new specialist smoking cessation service in the London Borough of Redbridge.
Photo by Markus Spiske on Unsplash
The new service will commence from 1 April 2023 and will be operational for an initial three-year term. It comes as an addition to WDP’s well-established adult and young people’s substance misuse and sexual health services in the borough.
The service will provide confidential, evidence-based behavioural and pharmacological advice and support to those who live, work or study in Redbridge, aged 12 and above, to help them to stop smoking or using other forms of tobacco.
The new service brings with it WDP’s commitment to co-production and working in close partnership with the areas it serves. It will also have a keen focus on accessibility and supporting priority populations including those who use non-traditional and smokeless forms of tobacco, pregnant women, young people, and people who are engaged with mental health services. This will be supported by regular consultation with service users and community and faith groups.
With a main hub in Ilford, the service will be embedded in the community, delivering a wide range of satellites and outreach activities in locations such as GP surgeries, COPD clinics, inpatient wards, mental health services, pharmacies, and other community sites. The team will be able to provide digital and remote contact, and WDP’s valued community pharmacy partners will also be able to provide smoking cessation interventions, supported by WDP’s chief pharmacist. This will ensure the service has a wide variety of accessibility options to reduce barriers to accessing support.
Gladys Xavier, director of public health for the London Borough of Redbridge said, “Smoking remains the leading causes of preventable illness, premature death and health inequalities. The new service will deliver a flexible and accessible service working closely with our NHS partners and will proactively outreach with our underserved communities to support residents to quit smoking and tobacco.”
Craig Middleton, executive director of services at WDP added, “This is an exciting new development for WDP and we are delighted to be delivering a specialist smoking cessation service to the residents of Redbridge. At WDP we are passionate about supporting people to improve their health and wellbeing and this is a perfect opportunity for us to support more people to do just that.”
This post was originally published by WDP. Read it here.
DDN magazine is a free publication self-funded through advertising.
We are proud to work in partnership with many of the leading charities and treatment providers in the sector.
Launch of Drink Drug Hub website provides reliable harm reduction information for anyone in North Yorkshire.
Not every person who drinks or uses drugs develops harmful patterns of use – but drink and drugs can cause lots of people lots of problems.
By providing reliable and accurate information, we can help adults and young people makemore informed decisions, understand how to access support, and potentially reduce the harms they face. We can help family and friends feel less alone. We can help professionals feel more confident to talk about drugs and alcohol and provide effective support.
Drink Drug Hub has been developed by North Yorkshire Horizons, the county’s community drug and alcohol service.
The website, which can be found at www.drinkdrughub.co.uk, presents an extensive but easy to use database of articles, videos and fact sheets. Resources cover everything from alcohol and prescription medications to illicit drugs like cocaine and heroin.
Anyone in North Yorkshire can also attend free training or awareness events, and practitioners can discover learning opportunities provided by other agencies across our region. Sessions will cover topics like an introduction to drugs/ alcohol and administering naloxone, a life-saving medication that can reverse the effects of an opioid overdoses.
Prior to launching the site, people who use alcohol and other drugs, and experts in the field of treatment, recovery and harm reduction gave feedback on the content, effectiveness and usability of the website to North Yorkshire Horizons.
The Office for National Statistics recently revealed that 2021 was the worst year on record for both drug related deaths and alcohol related deaths in England and Wales. Equipping people with knowledge about substances is an important way to reduce the harms that drugs and alcohol can cause.
Louise Wallace, Director of Public Health at North Yorkshire County Council, said: ‘Drink Drug Hub is a really important resource for our communities. It will help to equip people across North Yorkshire with reliable information and will also allow our communities to engage with awareness sessions delivered by experts, and practitioners working in our services to book onto and attend training to develop their own knowledge and skills.’
Lee Wilson, Regional Director at Humankind, the national charity which runs North Yorkshire Horizons, said: ‘We believe that people deserve to have access to accurate and up-to-date information about the drugs they take, and that’s why our team have worked so hard to create Drink Drug Hub. We’re excited to launch this new resource, which we know can improve health outcomes in North Yorkshire, and potentially save lives.’
Matt Bee, Specialist Training Facilitator at North Yorkshire Horizons and Drink Drug Hub project lead, said: ‘We know that people are often overwhelmed by the amount of information available online about alcohol and other drugs, and it can be difficult to know what sources to trust. Our goal is to make it easy for people to access reliable information verified by experts, so that they can be empowered to make the best decisions for their own health and wellbeing, and that of their loved ones.’
Almost 50 leading health experts have written to the chancellor urging him to increase alcohol duty when the current freeze ends later in the year.
MP Dan Carden has talked openly about his own issues with alcohol.
Among the signatories are Dan Carden MP and the chief executives of Alcohol Change UK, Humankind, Nacoa, and the British Liver Trust, as well as the president of the Royal College of Surgeons and the chair of the Royal College of General Practitioners.
A decade of cuts and freezes to alcohol duty have seen alcohol become 14 per cent more affordable since 2010, the letter states, which has ‘undoubtedly’ contributed to the current record numbers of alcohol-related deaths. Alcohol-specific deaths in the UK reached their highest ever level in 2021, at more than 9,600 – a 27 per cent increase in just two years. When the ‘alcohol duty escalator’ – the annual 2 per cent increase above inflation – was in place, deaths of alcohol-related liver disease fell, the letter states.
Sir Ian Gilmore: ‘record-breaking rates of harm cannot be ignored.’
The current rate of inflation means that while the price of beer has risen by just over 5 per cent since 2010, and wine by just 2 per cent, the price of juice has risen by almost 17 per cent over the same period, the letter points out. The decade-old estimate of a £3.5bn annual cost of alcohol harm to the NHS in England alone is likely to be a ‘significant’ underestimate, it adds. ‘Increasing alcohol duty in the upcoming spring budget would help to alleviate pressure on the NHS and generate much needed income,’ said Alcohol Health Alliance chair Sir Ian Gilmore.
‘Moreover, if the chancellor builds automatic uprating into the duty system, he will ensure that his duty reform plans remain effective well into the future, protecting the lives of people today and for generations to come. As a former health secretary I’m sure he will appreciate the damage alcohol harm does to communities, frontline services and the economy. Since 2019 we have seen a 27 per cent rise in deaths from alcohol and over 1m hospital admissions a year. These record-breaking rates of harm cannot be ignored any longer.’
Wednesday 1 November – Friday 3 November Liverpool
Club Health Liverpool 2023 is the 12th international conference on nightlife, substance use and related health issues.
The very first Club Health conference was held in the world famous Cream nightclub, Liverpool in 1997. Following the success of the event, The 1st International Conference on Nightlife, Substance Use and Related Health Issues was held in Amsterdam in 1999. Club Health conferences have since been held bi-annually in Australia, North America and throughout Europe. The 12th International Conference on Nightlife, Substance Use and Related Health Issues returns to Liverpool in November 2023.
Following a Leeds City Council procurement process, Forward Leeds has been successful in winning the contract to provide the city’s alcohol and drug support service for at least another five years.
The service, with sites in Armley, Seacroft and the city centre, will begin its new contract on 1 April 2023. The initial contract will run until 31 March 2028, with Leeds Council having an option to extend after that date for up to five years, potentially taking it up to April 2033.
Forward Leeds, who recently won Leeds City Council’s Partner of the Year, is a consortium between three charities: Humankind, St Anne’s Community Services and BARCA-Leeds along with the Leeds and York Partnership NHS Foundation Trust (LYPFT).
Councillor Salma Arif, Leeds City Council’s Executive Member for Public Health and Active Lifestyles, said, “As a Care Quality Commission outstanding rated service, it is really pleasing that Forward Leeds have been awarded this contract for the next few years. The service plays a vital role in addressing the challenges posed by drug and alcohol use to individuals and communities in Leeds, ensuring that anyone in the city struggling with drug and alcohol issues is able to get support.
“For some years now, Forward Leeds has consistently been one of the highest performing drug and alcohol treatment services in the country, and it is one of only a few services in the country that is rated outstanding by the Care Quality Commission (CQC)”.
Victoria Eaton, Director of Public Health at Leeds City Council, added, “It is fantastic news that Forward Leeds will continue to provide the Leeds City Council Public Health commissioned drug and alcohol service, which offers support for anyone affected by drug and alcohol use. The service has gone from strength to strength, to become one of just a few drug and alcohol services to be rated as outstanding, by the Care Quality Commission, in the country.”
Operations Director of Forward Leeds Helen Cook commented, “To be awarded the contract for at least another five years is fantastic. It reflects the quality and the hard work of the staff across our partnership and the commitment that they show in working with people who come to us for support.
“We have had to prove that we are able to continue to offer the high-quality service we have been doing and that we can develop and evolve our service to meet the ever-changing needs of the city.”
Humankind Regional Director Lee Wilson also said, “Having our contract renewed is a testament to the dedication of our staff and volunteers who provide the highest quality of care and support to everyone who comes to us needing help.
“The service has had to meet significant quality thresholds in the bidding process along with due diligence checks on safeguarding, health and safety, finance, and insurance. These were all completed successfully with no issues identified. Our social value response was even given the top score possible by the council.”
In North Yorkshire and York we’ve been building a practitioner network of multi-agency and multi-professional partners to support the sharing of dual diagnosis skills and knowledge across the region. As part of this work, we shared with DDN readers our joint pledge for working better together to promote collaborative service execution (DDN, February 2022, page 20), and we’ve been developing shared training opportunities with the hope of building collective confidence and competency in this area.
The Dual Diagnosis Network offers a shared space to support collaborative thinking.
It’s been wonderful to see the partnership between specialist substance misuse and mental health services grow and develop through regular forums, events, training, and open communication across the locality. We still have high aspirations about what we can achieve in North Yorkshire and York, and this work is our pledge going forward.
As part of this we identified that, while the process of collective learning in dual diagnosis is a priority, there is a continuing need for colleagues from different services to have shared spaces to talk, connect and learn together. The hope is that joint and collaborative working comes from not just service-level agreements and policy, but through relational connection and understanding of each other’s roles, culture, and values.
The Dual Diagnosis Network offers a shared space to support collaborative thinking and reflection from multi-agency partners such as mental health, drug and alcohol services, police, probation, third sector providers, housing, social care, advocacy providers and education. However, there’s an identified need for shared, focused learning events to support skills development across the region.
Training and supporting professionals to learn and develop their skills is essential and ensures individuals feel competent in what they do, which in turn supports improved clinical outcomes for service users. The implementation of any training strategy is, however, often fraught with complexity – as there are challenges around consistency, cost, application of learning and the return on investment. While tackling all these complexities and challenges is outside the work we’ve done, our approach to shared learning has supported people to learn and develop, fulfilling our overarching aim of helping clinicians from different services to come together and learn together to build better relationships. The aim is to model and support collaborative working on a clinician-to-clinician level.
As an example of the learning together approach, for the last few years we’ve held an annual dual diagnosis conference. This has been hosted online and is open to all in the region, with a focus on developing understanding and knowledge for those both experienced and less experienced in working with service users with co-existing needs. One of the main aims of the Dual Diagnosis Network and conference is to engage people from mental health and drug and alcohol services in a way of working and learning that will benefit the people we work with.
The dual diagnosis webinar focused on several clinical areas including developments in prescribing, lived experience perspectives on dual diagnosis and recovery and trauma-informed care, as well as break-out room discussions on partnership working for better outcomes and how we can develop a greater sense of collaborative connectedness for services and service users.
Using live engagement software, we were able to collect data throughout the conference about who was in the room, their insights and their feedback. The data revealed that we had a varied mix of professionals, from more than 25 organisations and services. Results on the day showed us that, overall, attendees came away having learnt a lot about the shared topics, with individuals sharing service pathways with each other as well as concerns with commissioners and senior staff that they might otherwise have found hard to express.
The Dual Diagnosis Network, and more specifically the annual conference, has allowed for spaces where passionate people working in the mental health sector, drug and alcohol support and wider services come together to interrogate and co-create shared ways of learning. What has also developed, however, is a process of better service connection. This way of connecting and its growth has supported us all to begin creating a shared professional movement to facilitate change in a steady and meaningful way. By being more systemically connected we support our service users together – and better.
Dolly Cook is area manager and co-chair of the Dual Diagnosis Network, Changing Lives.
Dr Stephen Donaldson is clinical psychologist and co-chair of the Dual Diagnosis Network – Tees, Esk and Wear Valleys NHS Foundation Trust.
Kate McLaven is digital inclusion coordinator at Changing Lives, York Drug & Alcohol Service
Local authorities in England will receive £421m for drug and alcohol treatment services through to 2025, the government has announced. More than 150 councils are being allocated funding, which includes £154.3m for 2023-24 and ‘indicative funding’ of £266.7m for 2024-25.
The funding will help get more people into treatment and enhance the quality of treatment on offer, says government
The money will help to enhance the quality of the treatment on offer, support more people leaving prison into treatment and allow the recruitment of more treatment staff, the government states, with more people benefitting from residential rehab and inpatient detox services. The funding is part of the government’s commitment to ‘significantly’ increase treatment capacity as part of its 2021 drug strategy, it says, and estimates that over the first three years of the strategy the additional investment will ‘prevent nearly 1,000 drug-related deaths – reversing the upward trend in drug deaths for the first time in a decade.’
The funding follows the £94.5m made available for 2022-23 and the recent announcement of £53m to improve housing support (www.drinkanddrugsnews.com/government-pledges-housing-support-cash-for-areas-most-in-need). Areas with the highest need have been prioritised, the government says, based on the size of their treatment populations, drug-related death rates, opiate and crack prevalence, and crime and deprivation.
Continued investment is crucial to a world class treatment and recovery system, said Prof Dame Carol Black
‘This continued investment is very welcome and will be crucial in supporting local authorities and their partners to increase the capacity and quality of their services for people with drug and alcohol dependence, in line with the key recommendations of my independent review of drugs,’ said Professor Dame Carol Black. ‘This will help realise the ambitions of the government’s ten-year drug strategy, to deliver a world-class treatment and recovery system, reduce drug use and drug related crime, and save lives.’
‘Drug misuse has a massive cost to society – more than 3,000 people died as a result of drug misuse in 2021,’ added health and social care secretary Steve Barclay. ‘This investment in treatment and recovery services is crucial to provide people with high-quality support, with services such expanding access to life-saving overdose medicines and outreach to young people at risk of drug misuse already helping to reduce harm and improve recovery. This funding will help us build a much-improved treatment and recovery service which will continue to save lives, improve the health and wellbeing of people across the country, and reduce pressure on the NHS by diverting people from addiction into recovery.’
The announcement has been welcomed by organisations across the sector:
‘Today we have certainty over the funding situation for the next two years which means that, as a sector, we can plan for the future and focus on ensuring that services are accessible to anyone who needs support, building on the progress already made in joint working across mental health, criminal justice and treatment agencies and creating safer communities for us all.’ Clare Taylor, chief operating officer, Turning Point
‘Following the launch of the ten-year drug strategy, investment in services that support people using drugs has already started to make a difference on the ground, with the recruitment of additional frontline and clinical staff, and more people coming into treatment. Today’s announcement provides much-needed stability and certainty for local services and the people who use them.’ Nic Adamson, deputy chief executive, Change Grow Live
‘In 2021 the ten-year drug strategy From harm to hope heralded a significant step change for the treatment and recovery system. We are now over a year on and, despite the challenges of the last 12 months, the strategy is beginning to make a difference. We welcome the government today continuing to unlock new investment to support people facing substance misuse, who are amongst our communities’ most vulnerable and stigmatised members. Now is the time to press on with the transformational, whole-system approach advocated by Dame Carol Black and set in motion by the drug strategy.’ Lea Milligan, chair, Collective Voice.
‘We welcome the confirmation of local authority funding for vital, evidence-based drug and alcohol treatment and recovery services. Dame Carol Black laid out an ambitious vision of how, as a society, we can rebuild our treatment and recovery services to help those most in need. Funding from the ten-year drug strategy, that brought Dame Carol Black’s vision to life, has already supported us to develop our services in areas with the greatest need.’ Paul Townsley, chief executive officer, Humankind
‘We hope that the additional £421m funding allocated to local authorities across England will be utilised to shape a joined-up system that ensures everyone in need has equal access to high-quality care. This cannot be achieved without partnership work across the sector, something that we are committed to doing as an alliance of NHS Trusts, in a continued effort to reduce the rising number of drug-related deaths seen annually and positively change the lives of thousands of people.’ Danny Hames and Kate Hall, chair and vice-chair, NHS Addictions Provider Alliance
National Apprenticeship Week (7–13 February) was a week-long celebration of apprenticeships in England.
The theme this year is ‘build the future’, reflecting how apprenticeships can help individuals to develop the skills and knowledge required for a rewarding career, and help organisations to develop a talented workforce.
To mark National Apprenticeship Week, WDP Merton Service Manager Helen O’Connor and former apprentice Elil Jeyakumar share how Elil has helped the service to break down the barriers to drug and alcohol treatment in the local Tamil community.
When WDP became the service provider for Merton in 2018, one thing we were keen to do was to respond better to local needs and deliver more culturally informed support to residents from Merton’s diverse communities. A particular area of focus was how the service engaged and worked with residents from the local Tamil community.
It can be difficult for professional interpreters who are not experienced in the delivery of drug and alcohol services, to understand our processes or find words to translate some of the vocabulary that we routinely use. Even when interpreters can support assessments and 1-2-1 keyworking sessions, their presence may be a barrier to an effective working relationship between a practitioner and service user. This is especially the case if there is a different interpreter in each session, or when the interpreter is from the service user’s community, if they do not feel confident speaking freely in front of them.
We wanted to find new ways to address barriers and to provide more choice in the solutions on offer, including groups and peer support. Using the apprenticeship levy scheme, we recruited an apprentice practitioner who could speak Tamil. Their role focused on helping us to understand how we could adapt to better engage with Tamil-speakers and their families, improving their experience of treatment.
Elil joined us in 2019. He has made such a difference to our local service and has now successfully completed his apprenticeship. We’re delighted that he has stayed with the service, becoming a fully-fledged recovery practitioner and a vital and valued member of our team. I’ll let him tell you more about his experience with us!
I am delighted that it is National Apprenticeship Week, and Turning Point we’re celebrating with a variety of events from webinars for future learners and managers to the launch of our apprenticeship community, writes a team member who started out as an apprentice.
We will hold our first Apprenticeships Graduation & Awards ceremony at the end of the week to recognise programme participants and graduates, as well as the managers who have contributed to the success of our apprenticeship programme.
Turning Point and apprenticeships
Turning Point apprenticeships are designed to support and nurture people in reaching their full potential, whether that is a management path or a sidestep into an area of interest.
Turning Point has been utilising apprenticeships for our existing workforce and how we can upskill the future leaders within the organisation within various apprenticeship standards and disciplines within the workplace. Apprenticeships require functional skills in English and Math, which may not have been achieved in school. Turning Point collaborates with our providers to assist colleagues in completing their function skills prior to or concurrently with their apprenticeship.
Our primary focus has been on developing our front-line teams through care and management apprenticeships ranging from level 2 to level 7. This has given 117 Turning Point colleagues who have/will have a recognised qualification.
To date, Turning Point has completed 55 apprenticeships, with our national average of 85% achieving a Merit or Distinction.
My apprenticeship journey
From my own personal experience of completing my own apprenticeship during Covid 19, the Turning Point approach is about supporting and developing our people to achieve success.
Turning Point and the provider’s assistance was critical for me. I had a mentor to whom I could turn for advice, and I had regular phone calls with my tutor to ensure I was on the right track. Working with the team also provided me with opportunities to be a part of projects that I would not have been a part of prior to beginning my apprenticeship.
As a result of completing my apprenticeship, I have gained additional responsibilities such as National Apprenticeship Week and the apprenticeship programme. Examining Turning Point’s strategic approach to apprenticeships and professional development. I have close working relationships with managers, learners, and providers, and what I enjoy most about my job is seeing how colleagues progress and achieve. Particularly during their learning stage. Seeing them overcome a challenge and seeing their confidence grow.
Find out more about the benefits of Turning Point’s apprentice schemes here.
DDN magazine is a free publication self-funded through advertising.
We are proud to work in partnership with many of the leading charities and treatment providers in the sector.
There has been a ‘doubling’ of drug-free wings in prisons, the government has announced. ‘New incentivised substance-free living units’ are now operating in 45 jails in England and Wales, it says, with up to 100 special blocks planned by 2025 alongside special abstinence-based recovery wings.
The aim is to reduce the risk of reoffending
The incentivised units feature regular drug testing as well as ‘substance misuse courses’, while the government is also investing in up to 18 drug recovery wings where prisoners will receive six months of intensive abstinence-based treatment, it says. The aim of both the incentivised units and recovery wings is to reduce the risk of reoffending, the government states, and ‘will make sure prisons are places where criminals get – and stay – clean while they pay their debt to society, instead of languishing on drug substitutes like methadone which can hinder their rehabilitation’.
The incentives for prisoners include extra time out of their cells and more education and work opportunities, and ‘once they’ve turned their back on drugs for good’ – including any substitution medication – they will have the opportunity to be transferred to a recovery wing. Funding for the incentivised units and recovery wings comes from the financing already allocated as part of the ten-year drug strategy.
Reducing supply is not enough to break the cycle of addiction and offending,’ said justice secretary Dominic Raab
A 2020 report from the Reform think tank found that the number of prisoners saying they’d developed a drug problem while in prison had doubled since 2013-14, to almost 15 per cent of all prisoners, with a ‘significant’ impact on levels of violence.
‘We are clamping down on drugs behind bars with tough new security, but we know reducing supply is not enough to break the cycle of addiction and offending,’ said justice secretary Dominic Raab. ‘Our new drug-free units and drug recovery wings will help prisoners tackle their addictions, including to opiate substitutes like methadone, in turn cutting their risk of reoffending and creating safer streets.’
National Apprenticeship Week 2023 takes place from Monday 6 February to Sunday 12 February. With both Dame Carol Black’s Independent Review and the national drug strategy, From Harm to Hope, singling out workforce development as a national priority and essential criteria for success, Humankind is taking the opportunity to highlight the achievements and aspirations of the 45 apprentices at our charity.
Photo by John Schnobrich on Unsplash
Across our County Durham Drug and Alcohol Recovery Service, Liaison and Diversion, and Crisis teams, there are 15 apprentices with lived experience of drug and alcohol use, recovery, mental health, or experience of the criminal justice system completing a Level 2 in Adult Care.
These apprentices were specifically recruited for their unique experiences, each bringing empathy, understanding and a range of skills to the role, which benefits the people accessing these services, our national charity, and the wider charity sector.
Ben Fidler, a Peer Apprentice in recovery in the County Durham Drug and Alcohol Recovery Service, shared his journey, from volunteering to his apprenticeship, and how it increased his self-confidence.
“Humankind’s positive approach to interviewing makes you feel like they are wanting to learn about you and your worth as a person,” Ben commented. “They go the extra mile to find the right person, and it feels great when that person is you! It is a really refreshing outlook.”
Another apprentice with lived experience commented that, “I have always been passionate about mental health and helping others, and through this apprenticeship, being able to help others makes me feel there is a more positive outcome from my own experiences.”
We have seen great success within our apprentice programme. Nine out of 16 who started in entry level positions after completing Level 2 or 3 apprenticeships are still employed in permanent positions. The apprenticeships have provided the others with the tools to make a positive impact in new roles.
George Bell began his journey with us as a volunteer before becoming a Peer Support Apprentice in March 2020. He described his apprenticeship experience as a great way to learn new skills and knowledge while being part of the team, and excelled in his role, securing a permanent position first as a Peer Support Worker and now as Peer Mentor and Volunteer Coordinator in the Tees Crisis Team.
Of his experience, George said, “The wider team were all very supportive and encouraging which is great for confidence building and also getting great shadowing experiences with different members of the team.”
Each apprentice at Humankind participates in on-the-job learning to gain the skills and experience required to develop their career within a supportive environment. Their work makes a real difference to the lives of people we support every day.
The programme covers a range of apprenticeship standards, including Adult Care, Finance and Customer Service among others. The apprenticeship standards studied support our different services across the country, from community drug and alcohol treatment to corporate services.
As well as apprenticeships for people looking to begin their career journey within the charity sector, over half of the apprenticeship learners were already employed by us and requested to complete an apprenticeship for their own personal development.
This includes 11 managers studying towards a Level 5 apprenticeship in Operations Management with Activate Business School. Feedback so far has been positive, and the organisation will support more managers to study towards the Level 5 Operations Management apprenticeship in the future. The apprenticeship is delivered remotely, fitting around the workdays of the learners.
Roxanne Dark, Service Manager at Humankind’s Staffordshire Treatment and Recovery Service (STARS) said, “The level 5 apprenticeship has given me the ability to stay in the role I enjoy while working towards my future in the same working environment. It has helped me in my role as I feel I am a better manager and I think in different ways now.”
We work with seven different training providers who deliver apprenticeships in varied ways, including with online platforms and face-to-face learning in a higher education or workplace setting.
In addition to Activate Business School, these providers include Darlington College, East Durham College, Impact Futures, Kaplan Financial Ltd, New College Durham, and Teesside University.
The apprenticeship programme is overseen by Humankind’s Talent Development Manager, Katie Woodward. Katie’s role involves developing the apprenticeship offer while working closely with services to identify current and future workforce trends.
“The most rewarding part of the role,” Katie said, “is the opportunity to support our workforce, from volunteers to managers, to develop their skills and careers every day.”
Despite the best efforts of the sector, we are all aware that deaths from drug poisoning have reached record levels in England and Wales, with 4,859 deaths registered in 2021. This is the highest number since records began, and almost 50 per cent of those deaths involved an opiate. Without the harm reduction interventions of providers like Turning Point, the situation would be significantly worse, but we see that there is still a long way to go and that we need to work differently.
On 30 November last year Turning Point hosted its first Safer Lives conference, supported with an education grant from Ethypharm. Held in Birmingham, our aim was to bring together commissioners, public health officials, third-sector organisations and our partners in the sector to join in making a commitment to addressing the drug death crisis.
We welcomed around 100 delegates from third sector and NHS treatment providers, local authority public health teams, the police, ambulance services and organisations working with people who are homeless. From across the drug and alcohol sector colleagues from CGL, With You, Humankind and Cranstoun were in attendance, and it was inspiring to see so many people from different organisations coming together for a common goal.
In my role as Turning Point’s national safer lives lead, I co-chaired the conference with our clinical director Dr David Bremner. After working in harm reduction for many years I joined Turning Point in 2020 as harm reduction manager for our Somerset service, and when I was offered the opportunity to expand this harm reduction work as national safer lives lead I jumped at the chance. The role allows me to support Turning Point in our increased focus on harm reduction while working across our services to increase naloxone awareness, distribution, and carriage. I plan to put lived experience at the centre of what I do and one of my first aims is to expand our peer-led naloxone distribution programme.
I often hear that there is too much focus on naloxone, that we need to look at benzos, people using alone, and the case for overdose prevention sites. And of course we do. But making sure naloxone is in the hands of everyone who may need to use it is vital. Professionally I’ve administered naloxone multiple times, but for me this is personal. I wouldn’t be here if it wasn’t for naloxone. I have lost friends who might still be here if naloxone had been more widely available. That’s why, at the start of the conference, I asked everyone in attendance to get trained and pick up a naloxone kit if they didn’t already have one. Turning Point staff provided this training throughout the conference and by the end of the day had issued more than 60 kits.
Speakers on the day included Professor Dame Carol Black, independent advisor to the government, Dr Ed Day, national recovery champion, and Pete Burkinshaw, alcohol and drug treatment and recovery lead at the Office for Health Improvement and Disparities (OHID). The conference gave us the opportunity to reflect on where we are as a sector, and what the future may hold, and listen to examples of innovative practice in naloxone distribution from colleagues.
Professor Dame Carol Black reflected on the progress made since she published her report on the sector. She reminded us that the current economic uncertainty means we need to be ‘bold, determined and innovative.’
The most moving presentation of the day came from Abigail Kearley, Turning Point’s national service user involvement lead. She spoke on behalf of Julie Rose, a mother who tragically lost her son to a heroin overdose. On a day when we were presented with a lot of statistical information this was a powerful reminder of the real people those numbers represent.
Julie McCartney and Lauren Sloey from the Scottish Ambulance Service discussed their role in widening the provision of naloxone (40 per cent of those receiving a kit were not in treatment) and George Charlton spoke about his own experiences of childhood trauma and drug use, the stigma experienced by people who use drugs, and how this led to his development of multiple peer naloxone programmes.
For the final session of the day, I joined the workshop presenters for a panel Q&A session. Delegates used this opportunity to ask the panel for practical tips on extending the availability of naloxone, and questions included how to engage the whole drug service team in the supply of naloxone, how to get more pharmacies on board, and why it isn’t mandatory across England, Wales and Northern Ireland for all police officers to carry naloxone.
Our aim for the day had been achieved. We had come together and shared learning and innovation, and I hope all left with ideas and inspiration to carry forward in our work. Two clear messages stood out from the day – the importance of collaboration and the sharing of knowledge, and the need to collaborate with those who are best placed to get naloxone to people furthest from treatment services. Whether that be the ambulance service, A&E departments, the police or those with lived and living experience, we need to work in partnership if we want to reduce these tragic and avoidable drug deaths.
Deb Hussey is national safer lives lead at Turning Point
——-
USING INSIGHT FROM PEOPLE WHO USE DRUGS TO INCREASE CARRIAGE RATES
Dr Jenny Scott, Bristol University
Dr Jenny Scott, a researcher from Bristol University who also works for Turning Point as a non-medical prescriber, spoke about a project that aims to identify barriers to carrying naloxone and develop solutions to overcome them. In Somerset a group of Turning Point service users worked with staff and university researchers to look at barriers to naloxone carriage.
They identified three key areas. One was the practical issue of carrying a kit that some felt was bulky, with a possible solution widening the availability of naloxone nasal spray. Another was the risk of being identified as someone who uses drugs – they felt a campaign to widen naloxone accessibility and acceptability to the general public would go some way to address this. The third issue was availability – not everyone lives near a local provider, particularly in rural areas, and not everyone knows other places they can get a kit.
——-
NALOXONE AND THE POLICE
Chief inspector Jason Meacham
Chief inspector Jason Meacham from Durham Police gave a presentation on the introduction of naloxone in police custody suites. Asked about opposition in some forces to officers carrying naloxone, he said he felt these concerns were unfounded but that he would be happy to contact any officers to discuss their objections. Having recently implemented a police naloxone pilot for Turning Point in Somerset, I was able to share my experience of the challenges we faced and how we overcame barriers to go on to train and issue naloxone to almost 150 officers. It was such a positive end to the conference and made me optimistic that there would be very real outcomes from the day.
National Apprenticeships Week is a time to celebrate the brilliant work of apprentices and all that apprenticeships have to offer, says The Forward Trust’s Executive Director of Employment Services, Asi Panditharatna.
Welcome to National Apprenticeships Week 2023! Join us in celebrating the brilliant work of apprentices, their employers and the families that support them.
This year’s theme is Skills for Life, focusing on how apprenticeships can increase the confidence, skills, knowledge, and behaviours needed to succeed in a job and career.
At a time of growing economic uncertainty, with more jobs requiring higher levels of education, apprenticeships are a valuable way to build the skills and knowledge that can often lead to a rewarding career, with better levels of pay and benefits.
In our experience as a leading Adult Education Budget provider, learners we have supported into apprenticeships frequently access better paid, more stable and exciting employment opportunities. Our employers and providers support learners to start apprenticeships by providing awareness sessions, practice interviews, work trials and often roles paying a Real Living Wage.
Through our Prison Apprenticeship Pathway, funded by Porticus UK and working in partnership with apprenticeship providers such as Umbrella Training, we also support prison leavers into high quality apprenticeships in hospitality, a potentially vital step in someone turning their life around.
This week, we are celebrating our achievements delivering the Employability Practitioner Standard (Level 4), an exciting programme of learning that helps up-skill professionals working in the employability sector. We look forward to sharing some first-hand experiences of our inspiring apprentices.
In 2023, we are planning to expand our Employability Practitioner apprenticeship within the voluntary, community and social enterprise sectors as well as local authorities that are delivering employability support and information, advice and guidance (IAG) services. Watch this space!
Head of Clinical Intervention at Phoenix Futures, Gabrielle Epstein
As Head of Clinical Intervention at Phoenix Futures, Gabrielle Epstein has been at the forefront of developing the approach for blended substance use and mental health provision at New Oakwood Lodge, a new CQC–registered Therapeutic Community, based in Derby.
Tell us about New Oakwood Lodge and what needs it is seeking to address.
New Oakwood Lodge provides coordinated mental health and substance use care in one location. People experiencing co-existing mental ill health and substance use may struggle to access mental health treatment due to their substance use and struggle to access substance use treatment because of their mental health. People can become stuck unable to get the help they need where they live.
A residential placement, with appropriate detox, could be an answer for them as it enables people’s care to be coordinated in one location, but many rehabs lack the mental health treatment capability and are not set up to coordinate care across mental health and substance use needs nor do they provide a range of specific mental wellbeing activities.
This means that people with a co-existing interdependent need can struggle to access the care they need anywhere. They face a huge health inequality.
Accessing residential treatment requires a high level of organisation, support, and resilience. There are multiple assessments and appointments to attend which can be difficult for people who struggle to express themselves and find talking about traumatic life experiences triggering. We see people too easily labelled as ‘non-compliant’ or ‘unengaged’ when in fact a history of trauma may act as a barrier to sharing openly or anxiety may result in non-attendance at assessment sessions. People who lack support and confidence are disadvantaged.
Furthermore, if people can access rehab, then the unfamiliarity of the place, having to be with so many new people and talking about feelings so openly can be too much.
At New Oakwood Lodge the skills needed to support people excluded from other forms of support have been brought together in a multi-disciplinary team. Essentially, we’ve made accessing multiple forms of treatment (which can be incredibly complicated for some people to access) simple for everyone by delivering it in one place in a single treatment episode.
Can you talk us through the interventions on offer at New Oakwood Lodge?
The environment, protocols and treatment offering at New Oakwood Lodge are designed to provide the necessary support and interventions individually to maximise Community Members’ engagement in treatment.
The programme is based on the Therapeutic Community approach – people live together and learn from each other. The community helps individuals emotionally and supports the development of behaviours, attitudes, and values of healthy living. The structured group programme enables people to share and learn together in groups facilitated by expert staff.
Treatment incorporates 1:1 counselling utilising CBT to support mental health and substance use. Our Recovery through Nature programme enables people to come together with a common purpose to complete conservation tasks. Being with others, exercising together and working to create a positive environmental impact is proven to aid mental well-being. We bring together these core interventions, and other specialist interventions so that they fit together in a blended approach to care.
The team at New Oakwood Lodge is made up of a psychologist, counsellor, registered nurse and therapeutic workers in a multidisciplinary team supported by our Clinical Governance Committee headed up by a senior consultant psychiatrist. They work together across different disciplines of care to create an environment and milieu to deliver coordinated and personalised care bolstered by peer support.
What other approaches add to the Enhanced Environment at New Oakwood Lodge?
The length of treatment will typically be longer than usual due to an extended assessment and welcome/induction process at the start of treatment. We also expect the discharge period to be longer and more comprehensive.
We are currently working toward the Enabling Environments accreditation from the Royal College of Psychiatrists. We are a member of the Enabling Environment Network which has been set up to encourage and support services that wish to ensure that everyone thrives, succeeds, and achieves more positive outcomes.
We take a modern approach to mental health meaning that we treat people, not just conditions. We enable people to be themselves in the safe, open, and caring nature of the Therapeutic Community.
Can you tell us more about blended substance use and mental health care?
At New Oakwood Lodge we provide mental health care coordinated with drug treatment and vice versa. Mental health interventions are specific to individual needs and equip and empower people to feel included, safe, and able to receive and offer support to others.
Mental health interventions exist in a reciprocal loop with drug treatment. So that 1-2-1 behavioural interventions for depression, for example, focus on helping people engage with their peers in groups, and activities that make up the everyday routine of residential treatment. Similarly, the safe and caring community of the service is an ideal environment for people to practise what they learn from 1-2-1 CBT interventions for anxiety.
There are a number of targeted mental health outcomes that we aim to achieve with our blended approach for example, improvement in peoples’ mental well-being and health including treating anxiety and depression, reduction in mental health crises and suicide/self-harm attempts, improved retention, reduction in early leavers and a potential reduction in psychiatric medication
Alex Armstrong, Turning Point’s Acting Apprenticeship Lead, discusses his journey and work during National Apprenticeship Week.
I am delighted that it is National Apprenticeship Week. We’re celebrating with a variety of events; from webinars for future learners and managers to the launch of our apprenticeship community. We will hold our first Apprenticeships Graduation & Awards ceremony at the end of the week to recognise programme participants and graduates, as well as the managers who have contributed to the success of our apprenticeship programme.
Turning Point and apprenticeships
Turning Point apprenticeships are designed to support and nurture people in reaching their full potential, whether that is a management path or a sidestep into an area of interest.
Turning Point has been utilising apprenticeships for our existing workforce and how we can upskill the future leaders within the organisation within various apprenticeship standards and disciplines within the workplace. Apprenticeships require functional skills in English and Math, which may not have been achieved in school. Turning Point collaborates with our providers to assist colleagues in completing their function skills prior to or concurrently with their apprenticeship.
Our primary focus has been on developing our front-line teams through care and management apprenticeships ranging from level 2 to level 7. This has given 117 Turning Point colleagues who have/will have a recognised qualification.
To date, Turning Point has completed 55 apprenticeships, with our national average of 85% achieving a Merit or Distinction.
My apprenticeship journey
From my own personal experience of completing my own apprenticeship during Covid 19, the Turning Point approach is about supporting and developing our people to achieve success.
Turning Point and the provider’s assistance was critical for me. I had a mentor to whom I could turn for advice, and I had regular phone calls with my tutor to ensure I was on the right track. Working with the team also provided me with opportunities to be a part of projects that I would not have been a part of prior to beginning my apprenticeship.
As a result of completing my apprenticeship, I have gained additional responsibilities such as National Apprenticeship Week and the apprenticeship programme. Examining Turning Point’s strategic approach to apprenticeships and professional development. I have close working relationships with managers, learners, and providers, and what I enjoy most about my job is seeing how colleagues progress and achieve. Particularly during their learning stage. Seeing them overcome a challenge and seeing their confidence grow.
Benefits of apprenticeships
We’ve seen colleagues advance through the apprenticeship scheme, from support worker to senior support worker to team managers, running their own services by completing apprenticeships alongside their day job.
We have established clear career paths and opportunities for future growth for our colleagues. Individuals’ practises may vary greatly while on the programme, depending on what they are studying that month. They can apply their knowledge, skills, and behaviours to the work environment. We are also considering future apprenticeships, as well as participating in research groups and exploring new apprenticeships to help develop our teams and establish new working relationships with providers and universities throughout England.
Turning Point has also joined the Apprenticeship Ambassador Network and the Apprenticeship Diversity Champion Network, pledging to make apprenticeships more accessible and inclusive, as well as to improve our social mobility and reach out to a broader workforce.
Apprenticeships are helping develop the future for our workforce and this is the most exciting part to seeing colleagues progression.
Turning Point Medical Director, Dr David Bremner, shares the new Turning Point HIV Strategy and the organisation’s work during HIV Testing Week.
This week is national HIV Testing Week. Across the country, Turning Point services are working with partner organisations to run HIV testing events and calling on people to get tested and know their status.
This week we are also launching the Turning Point HIV strategy, the aim of which is to ensure everyone that Turning Point supports in our drug and alcohol and sexual health services can easily access testing, treatment and ongoing support for HIV.
We have made great progress in tackling HIV in the UK; however, there is more to do and drug and alcohol treatment providers have a key role to play if we are to meet the government target to end new HIV transmissions by 2030. HIV prevalence amongst people who inject drugs in the UK is low but estimates suggest the risk of contracting HIV for this group is 22 times greater than for the population as a whole. People who inject drugs can be marginalised, they can face barriers to accessing services and are more likely to be diagnosed late.
Testing is quick and easy. Most tests come back negative, but it’s always better to know. If you test positive, it’s important to know you can live a long and fulfilling life with HIV. There’s support available to help you comes to terms with a positive diagnosis and modern HIV treatment means you can’t pass it on to others.
We consulted with people living with HIV, staff and partner organisations in developing the strategy which is guided by three underlying principles:
• Challenging stigma surrounding HIV within services and beyond. This will be achieved through the provision of robust staff education and training, and by providing clear information regarding HIV for people supported by our services.
• Ensuring key messages relating to HIV testing and treatment are clearly communicated. It is important that we achieve wider understanding regarding the fact that when HIV is diagnosed and properly treated it is undetectable and untransmissible.
• Ensuring all of our services are a safe space in which people we support who are living with HIV can access support and discuss their diagnosis and treatment.
We have lots of examples of good practice within services and over the coming period we will be focussed on sharing the learning from these – improving training for staff, the quality of information, advice and support we provide and our work with partner organisations. We are part of the generation that will stop HIV.
This year marks the tenth anniversary of Dry January. But are those who are least likely to take part – older people – the ones who would most benefit? DDN reports.
According to research published by Alcohol Change UK at the end of December, around 8.8m people – roughly one in seven UK adults – were planning to take part in Dry January this year. How many actually made it to the end of the month without a drink is of course a different matter, but the figure shows how firmly established the campaign – now in its tenth year – has become.
It comes as alcohol-related deaths and hospital admissions continue their upward trajectory. There were 280,000 alcohol-specific hospital admissions in England in 2019-20, while the broader measure that includes a secondary diagnosis linked to alcohol saw almost 980,000 – one in 20 of all admissions.
According to the latest ONS figures, meanwhile, 2021 saw alcohol-specific deaths across the UK reach their highest-ever level at more than 9,600 – a 7 per cent increase on 2020 and almost 30 per cent higher than 2019. Again it’s worth remembering that these figures only include deaths that are the result of conditions ‘wholly attributable’ to alcohol – primarily alcoholic liver disease – and according to ONS are therefore likely to account for only a third of all deaths that could be considered alcohol-related.
As usual, the alcohol-related death rate for men was far higher than for women, but what has changed in recent years is the age of those likely to be drinking the most. While the popular perception of ‘binge drinkers’ still tends to be of groups of people in their teens and twenties stumbling around town and city centres, according to the latest Health survey for England the people most likely to drink more than the weekly guidelines are now men aged between 55 and 74 and women aged 45 to 64.
Generational shift
One key reason for this generational shift in drinking patterns is that these are people who grew up at a time when excessive drinking was seen as the norm, with habits long-since becoming ingrained – especially as most of their friends are likely to drink at similar levels. ‘It’s those influences that the baby boomer generation had – that whole alcogenic environment,’ consultant old-age psychiatrist and visiting research fellow at South London and Maudsley NHS Foundation Trust, Dr Tony Rao, tells DDN. ‘It’s a combination of peer pressure, habit and lifestyle, and if you put all those into the mix you’ve got a generation that’s not ready to look at anything beyond that.’
Covid impact
COVID has also had a significant impact on drinking patterns, with research from a range of organisations coming to essentially the same conclusion – that while many moderate drinkers reduced their consumption during lockdowns and the pandemic as a whole, many of those who were already drinking too much began drinking even more. Researchers have warned that this is likely to cast a ‘long shadow’ on health, with a report from the University of Sheffield stating that it could lead to 25,000 additional deaths and almost 1m hospital admissions over the next 20 years. And again, it’s often older people who are most affected. ‘During that period of lockdown, the percentage change in people drinking over 50 units a week was consistently higher among 65 to 74-year-olds, which is very surprising,’ says Rao.
While public health campaigners consistently urge the government to tighten up what are seen as the toothless regulations around alcohol marketing, most proposals to do so tend to focus on young people – as is reflected in the consultation being carried out by the Scottish Government at the moment, with its plans to tackle sports and events sponsorship and statement that marketing is ‘associated with an increased likelihood that children and young people will start to drink alcohol’. Given this ongoing generational shift in drinking patterns, are they maybe barking up the wrong tree?
‘Definitely,’ Rao states. ‘We had the Drink Wise, Age Well project that lasted for seven years, but what I think we urgently need now is a nationwide public health campaign to show older people not only the extent of the problem but also how they can play a part in their own harm reduction.’
While Dry January is very much based around people who are already health-aware, what’s needed with older people is something to raise that awareness of harm, he stresses. ‘I think older people still see this kind of mind shift among younger people as very woke, very nanny state, because they don’t appreciate the true extent [of the harm] – “It’s not my problem, it’s someone else’s problem.” There’s all this ONS data and the media stories around it saying that younger people are drinking less – and that’s all well and good – but what they’re not saying is that older people are drinking far more compared to the same generation 50 years ago.’
It’s an issue that has to be tackled on two fronts, he believes. ‘We need a public health campaign on alcohol-related harm, but we also need to develop clinical services so there’s better screening and brief intervention. Not just because it would help to catch things early, but it would help to give addiction services a better understanding of the extent of the problem.’ And within those services there needs to be a multi-disciplinary approach, he adds. ‘You need the medical side to look at mental health disorders, the nursing and psychology side to engage people in reducing stigma and opening up about their drink problem, and then you need the social focus on community integration and recovery. It can take decades to achieve that kind of thing.’
Does Dry January Work?
So does Dry January itself work, or is it just a way for people to think ‘I’ve done that, now I can go back to bingeing on 1 February?’ ‘There’s always this misconception with alcohol, because it’s such a stigmatising subject, that either you drink or you’re abstinent,’ he states. ‘But I think the longer-term impact for a large number of people is that it’s given them the chance to reflect on having healthier lifestyles and really looking at the part that alcohol plays in their lives.’ Alcohol Change UK, however, found that just 10 per cent of over-55s were planning to take part, a missed opportunity given they’ve often ‘been quite hedonistic, and are quite health-naïve’, he says.
While there’s obviously still large numbers of young people who drink heavily, it’s looking as though this overall shift in drinking patterns may well turn out to be permanent. One factor may be something as simple as alcohol not being seen as cool anymore among a growing proportion of younger people – for a generation whose every action is scrutinised on social media, getting drunk and losing control perhaps isn’t something particularly attractive. ‘I think there are three components,’ says Rao. ‘There’s seeing parents and grandparents who’ve suffered from alcohol problems, there’s the health aspect – they’re a much more health-aware population – and then there’s the cost of living. They can’t afford to – they’re probably more likely to go and have a craft beer every month than drink every week.’
Loud and consistent
In terms of where alcohol health campaigns should now be turning their focus, it doesn’t help of course that there’s been no alcohol strategy for a decade. And when one does finally come it’s highly likely to focus on young people, Rao points out. ‘So we need louder and more consistent voices for the older population, who are suffering. I really don’t think that at a political level, or a clinical level or a public health level, it’s really been taken seriously enough. I think the other reason is that there’s probably an attitude – not just among older people that they don’t want to change their habits – but among society as a whole of “why shouldn’t older people be allowed to enjoy themselves?”’ But what we know from definitive and robust reviews is that older people tend to do much better in terms of treatment and recovery than younger people. So it’s never too late.’ DDN


 The Listen, Believe, Affirm project came out of our work with the Centre of Expertise on child sexual abuse (CSA Centre). With their support, we carried out a survey across Change Grow Live to understand the level of skills and knowledge around child sexual abuse. We discovered that all of the tools were there – it was just a question of making sure those conversations happen. We needed to ensure that our staff felt comfortable and supported to ask the right questions, and that people were given the space to answer openly.
The Listen, Believe, Affirm project came out of our work with the Centre of Expertise on child sexual abuse (CSA Centre). With their support, we carried out a survey across Change Grow Live to understand the level of skills and knowledge around child sexual abuse. We discovered that all of the tools were there – it was just a question of making sure those conversations happen. We needed to ensure that our staff felt comfortable and supported to ask the right questions, and that people were given the space to answer openly. 

 We are proud to work in partnership with many of the leading charities and treatment providers in the sector.
We are proud to work in partnership with many of the leading charities and treatment providers in the sector.








 So what we decided to do at Cranstoun was create a pouch that contained enough equipment to support the person administering naloxone in one of these risky situations. We decided that our pouches should contain a number of useful items, which are kept together for ease of access.
So what we decided to do at Cranstoun was create a pouch that contained enough equipment to support the person administering naloxone in one of these risky situations. We decided that our pouches should contain a number of useful items, which are kept together for ease of access.  The passion the peer team bought to the table was quite amazing. You could really tell these pouches meant something personally to them. Without them, 2,000 would still be sat in boxes and I would be facing a telling off! So from me and all the people who now have a pouch, nice one PACKS – you did a mighty fine job on these!
The passion the peer team bought to the table was quite amazing. You could really tell these pouches meant something personally to them. Without them, 2,000 would still be sat in boxes and I would be facing a telling off! So from me and all the people who now have a pouch, nice one PACKS – you did a mighty fine job on these! 
 One thing we did notice when we were doing the naloxone training in public with the peer team was that sometimes people were interested in naloxone but didn’t have time to do the full training. So Deb from our Sutton service, the PACKS peer team and myself designed a Z-CARD which would contain all the key naloxone training information that could be given to someone with a kit. We know that if they read it they’ll have all the information needed to use the kit successfully.
One thing we did notice when we were doing the naloxone training in public with the peer team was that sometimes people were interested in naloxone but didn’t have time to do the full training. So Deb from our Sutton service, the PACKS peer team and myself designed a Z-CARD which would contain all the key naloxone training information that could be given to someone with a kit. We know that if they read it they’ll have all the information needed to use the kit successfully. 
 Watershed Moment
Watershed Moment Drilling into the detail – The Data
Drilling into the detail – The Data


 Anna Millington established a non-funded, non-affiliated support network for mothers who use drugs. It seeks to work collaboratively with professionals – on its own terms.
Anna Millington established a non-funded, non-affiliated support network for mothers who use drugs. It seeks to work collaboratively with professionals – on its own terms. We’re Not Going Away
We’re Not Going Away




 EDP has proudly supported people in the South West since 1984, and as a subsidiary of Humankind since April 2020. The two charities have worked closely together, with EDP drawing on Humankind’s national scale and expertise. As closely aligned charities, EDP will now take the next step in integration by merging fully into its parent charity on 1 July of this year.
EDP has proudly supported people in the South West since 1984, and as a subsidiary of Humankind since April 2020. The two charities have worked closely together, with EDP drawing on Humankind’s national scale and expertise. As closely aligned charities, EDP will now take the next step in integration by merging fully into its parent charity on 1 July of this year.









 The service will be delivered by the national charity Humankind which supported over 90,000 people in 2021/22. Humankind delivers four young people’s services and three family support services across London as part of its
The service will be delivered by the national charity Humankind which supported over 90,000 people in 2021/22. Humankind delivers four young people’s services and three family support services across London as part of its 













 The current evidence suggests that the harms associated with nitrous oxide (‘laughing gas’) are ‘not commensurate with control under the Misuse of Drugs Act 1971’, the ACMD has said in its updated assessment of the drug. The types of harms caused by nitrous oxide have not changed since the ACMD’s last report it 2015, it adds.
The current evidence suggests that the harms associated with nitrous oxide (‘laughing gas’) are ‘not commensurate with control under the Misuse of Drugs Act 1971’, the ACMD has said in its updated assessment of the drug. The types of harms caused by nitrous oxide have not changed since the ACMD’s last report it 2015, it adds.


 Central to our approach is a recognition that there are much-needed changes that we can take responsibility for. There are of course also many areas where we need to harness our collective influencing power, including how we might influence systems and policy change to drive improvements for women. Our presentation to the Drugs, Alcohol and Justice All-Party Parliamentary Group last month (DDN, February, p23) is an example of this work. To find out more about the group, check out our page on the Collective Voice website at www.collectivevoice.org.uk/womens-alcohol-and-drug-treatment.
Central to our approach is a recognition that there are much-needed changes that we can take responsibility for. There are of course also many areas where we need to harness our collective influencing power, including how we might influence systems and policy change to drive improvements for women. Our presentation to the Drugs, Alcohol and Justice All-Party Parliamentary Group last month (DDN, February, p23) is an example of this work. To find out more about the group, check out our page on the Collective Voice website at www.collectivevoice.org.uk/womens-alcohol-and-drug-treatment. 
 Women supporting women – stories from the frontline
Women supporting women – stories from the frontline 





 From the street
From the street

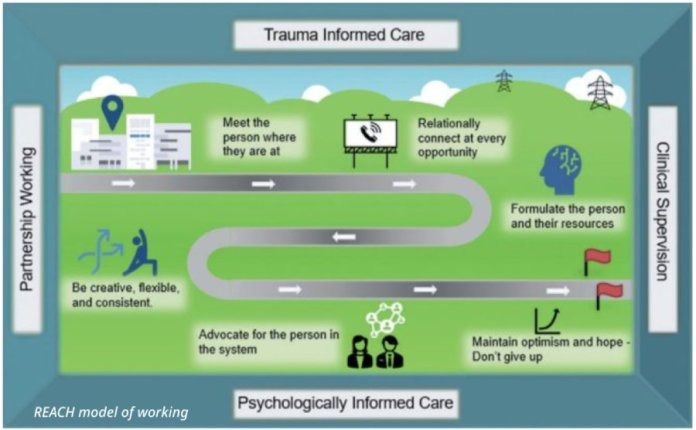












 The theme this year is ‘build the future’, reflecting how apprenticeships can help individuals to develop the skills and knowledge required for a rewarding career, and help organisations to develop a talented workforce.
The theme this year is ‘build the future’, reflecting how apprenticeships can help individuals to develop the skills and knowledge required for a rewarding career, and help organisations to develop a talented workforce. We will hold our first Apprenticeships Graduation & Awards ceremony at the end of the week to recognise programme participants and graduates, as well as the managers who have contributed to the success of our apprenticeship programme.
We will hold our first Apprenticeships Graduation & Awards ceremony at the end of the week to recognise programme participants and graduates, as well as the managers who have contributed to the success of our apprenticeship programme.




 In my role as Turning Point’s national safer lives lead, I co-chaired the conference with our clinical director Dr David Bremner. After working in harm reduction for many years I joined Turning Point in 2020 as harm reduction manager for our Somerset service, and when I was offered the opportunity to expand this harm reduction work as national safer lives lead I jumped at the chance. The role allows me to support Turning Point in our increased focus on harm reduction while working across our services to increase naloxone awareness, distribution, and carriage. I plan to put lived experience at the centre of what I do and one of my first aims is to expand our peer-led naloxone distribution programme.
In my role as Turning Point’s national safer lives lead, I co-chaired the conference with our clinical director Dr David Bremner. After working in harm reduction for many years I joined Turning Point in 2020 as harm reduction manager for our Somerset service, and when I was offered the opportunity to expand this harm reduction work as national safer lives lead I jumped at the chance. The role allows me to support Turning Point in our increased focus on harm reduction while working across our services to increase naloxone awareness, distribution, and carriage. I plan to put lived experience at the centre of what I do and one of my first aims is to expand our peer-led naloxone distribution programme. 







 While public health campaigners consistently urge the government to tighten up what are seen as the toothless regulations around alcohol marketing, most proposals to do so tend to focus on young people – as is reflected in the consultation being carried out by the Scottish Government at the moment, with its
While public health campaigners consistently urge the government to tighten up what are seen as the toothless regulations around alcohol marketing, most proposals to do so tend to focus on young people – as is reflected in the consultation being carried out by the Scottish Government at the moment, with its  So does Dry January itself work, or is it just a way for people to think ‘I’ve done that, now I can go back to bingeing on 1 February?’ ‘There’s always this misconception with alcohol, because it’s such a stigmatising subject, that either you drink or you’re abstinent,’ he states. ‘But I think the longer-term impact for a large number of people is that it’s given them the chance to reflect on having healthier lifestyles and really looking at the part that alcohol plays in their lives.’ Alcohol Change UK, however, found that just 10 per cent of over-55s were planning to take part, a missed opportunity given they’ve often ‘been quite hedonistic, and are quite health-naïve’, he says.
So does Dry January itself work, or is it just a way for people to think ‘I’ve done that, now I can go back to bingeing on 1 February?’ ‘There’s always this misconception with alcohol, because it’s such a stigmatising subject, that either you drink or you’re abstinent,’ he states. ‘But I think the longer-term impact for a large number of people is that it’s given them the chance to reflect on having healthier lifestyles and really looking at the part that alcohol plays in their lives.’ Alcohol Change UK, however, found that just 10 per cent of over-55s were planning to take part, a missed opportunity given they’ve often ‘been quite hedonistic, and are quite health-naïve’, he says.