As far back as 2002, research was showing that 70 per cent of people in drug services and 86 per cent in alcohol services had described or reported severe mental health problems in the previous year, said Dr Hauwa Onifade, a forensic psychologist at Turning Point involved in developing services with an integrated approach to co-existing mental health difficulties and substance use. Far too many in this client group were still failing to access the support they needed, she said.
Despite efforts to integrate services, there were ongoing barriers to bridging the gap. In many services there was ‘sequential delivery’, with clients told to address their substance issues before they could access mental health support, or parallel delivery – clients accessing both, but with difficulties in joining them up. Years of diminishing investment had taken its toll, while the transfer of public health functions to local authorities had also led to an ‘accountability gap’ across substance and mental health providers. ‘And of course COVID hasn’t made any of this any easier.’
High Risk
Turning Point had developed a substance use and mental health (SUMH) toolkit for professionals, condensing research and guidelines from PHE, NICE and elsewhere, she said. The organisation had also been working in Leicester, Leicestershire and Rutland on developing an integrated team, with a pilot launching during the COVID period following an audit of more than 3,000 clients. This had identified two significant groups where there were gaps in accessing treatment – populations involved in injecting drug use who were ‘frequent flyers’ at local hospitals and also presented with high levels of risk around mental health, including self-harm and suicide, and longer-term clients who, although there was little risk of self-harm or suicide, were in high levels of distress and unable to make changes in their substance use as a result.
‘We tend to focus on high-risk populations, almost to the detriment of the other group,’ she said. ‘And even with the high-risk populations we’re not necessarily working with them long-term, so they tend to fall into that pattern of re-presenting to services. A lot of services were involved in their care and a lot of people were aware of their difficulties, but they weren’t necessarily in treatment for very long.’
No Wrong Door
Turning Point’s integrated team had tried to implement the ‘no wrong door’ concept – that all services should have a fully open-door policy – along with a ‘huge focus on engagement and retention’, she told the seminar. There was also a need to focus on client needs rather than just diagnosis – ‘we found that when we focused on diagnosis alone we excluded a high number of clients who were struggling and in distress’.
Turning Point had also conducted a mapping exercise of all the services in the area that could meet the clients’ treatment needs. It found that specialist services for domestic violence, for example, would also work with people who had experienced those issues in the past, allowing the building of links to provide support while clients were on a waiting list. ‘Establishing those networks and looking at the wider availability of resources is really key,’ she said. ‘It’s astounding the number of peer support groups available’, and even organisations like Age UK could address issues of loneliness and provide interim support while clients waited to access other services. ‘So really broadening our idea of what intervention looks like for these client groups, which means we’re able to filter in a lot more options.’
Focusing on being able to deliver genuinely trauma-informed services was vital, alongside breaking down both stigma and professionals’ anxiety around their skill sets. Lack of clinical psychologists in third sector addiction services was a crucial issue, however – ‘I’m astounded by the number of services that don’t have psychologist input’ – and proper support for staff was also a key consideration. ‘If you’re working with people with those high levels of risk, as a professional you’ll likely need some support as well. Without that full structure and that supervision and training element, teams such as this would likely fall apart.’
But barriers didn’t just exist when it came to accessing treatment for co-existing conditions. There were also the legal barriers that prevented the use of substances that could provide potentially life-changing help for depression, anxiety, PTSD and other mental health issues.
Revolutionary
‘It was the first great revolution in psychiatry,’ said professor of neuropsychopharmacology at Imperial College London, David Nutt, of the widespread use of LSD therapy in the US in the 1950s and ’60s. There had been an ‘enormous clinical interest’ in LSD, and to a lesser extent psilocybin, with around 1,000 clinical papers and ‘overwhelmingly positive’ results describing safe and effective treatments.
For researchers and psychiatrists, psychedelics offered the opportunity to ‘ask questions of the brain that hadn’t been asked before, and potentially change brain function in a very positive way’, he said, and it was ‘remarkable’ how few adverse effects there had been. ‘Lower than you’d imagine for untreated populations at the time and certainly better than any treatment they were getting, which was essentially just barbiturates.’
It constituted a ‘remarkable period of enormous enthusiasm’, he stated. ‘But we don’t use them now, because in 1967 the US government decided to ban psychedelics because they thought they were encouraging the anti-Vietnam war movement.’ And – as ‘we’d always done in drug policy exactly what the US told us’ – the UK followed suit, as did the UN.
This meant an end to research, as it was almost always funded by governments, with even those researchers who could access funding from philanthropists unable to get hold of the drugs. It added up to ‘a genuine attempt by the US government and UN to eliminate all knowledge and almost all memory of the drugs, because they were seen as being so challenging to the status quo’.
In 2012, however, money finally became available from the Medical Research Council to study the use of psilocybin in treatment-resistant depression, dependent on an initial safety study. ‘But even that was easier than getting hold of the drug,’ said Nutt. ‘In the end, 32 months of our 36-month grant were spent on bureaucracy, which is all about protecting society from the dangers of magic mushrooms. It’s completely absurd.’
Pessimism bias
The study finally went ahead, involving 20 patients who had all failed to benefit from anti-depressants and CBT. ‘We gave them one dose, one trip of 25mg, and saw a halving of depression scores within a day.’ Even at six months there were still ‘huge’ effects, with some patients in remission after eight years. ‘It opened up the whole field, and now there are 40 different companies working in the field of psilocybin for depression.’
Psilocybin ‘changes the way people think’, he said, helping to remove the ‘pessimism bias’ involved in perpetuating depression. A subsequent ‘head-to-head trial’ of psilocybin versus the widely used SSRI antidepressant escitalopram found that psilocybin was ‘at least as good, and probably better’ on most measures, with ‘remarkably higher’ remission rates (www.drinkanddrugsnews.com/magic-mushrooms-may-be-as-effective-as-antidepressants).
While SSRIs worked by enhancing serotonin in the limbic system – ‘they are to depression what a plaster cast is to a broken leg’ – psychedelics worked in a different part of the brain by disrupting cortical thinking. This helped to break down negative thought patterns and increase wellbeing, without the blunting effect on the emotions that sometimes came with SSRIs.
Studies had now been widened to include areas like anorexia, OCD and pain syndromes, he said. These were ‘internalising disorders where people get locked into thinking patterns they can’t escape, and psychedelics can help them do that’. The drugs also worked well in treating addiction, he stressed, in that they helped to ‘break down the circuits that drive addictive thinking and habit behaviour’, and he was now involved in work looking at whether ketamine could be effective for behavioural addictions such as gambling or pornography.
Maximum benefit
MDMA was now likely to become approved therapy for PTSD in the US from the end of next year, he said. ‘They’ve done one phase 3 study, and the second one’s on its way – if it’s as good as the first I’m pretty sure it’ll get a licence, and hopefully we’ll then be able to use it in Britain. And maybe in the next three years we’ll be able to have psilocybin in the UK, depending on how the next phase 3 trial comes out.’ Psychotherapeutic support provided around the psilocybin dosing was essential, however. ‘I like the idea that we can bring psychotherapy and pharmacology together to maximise the benefits for people.’
‘As George Bernard Shaw said, “Those who cannot change their minds cannot change anything”, and I think what’s pretty clear is that psychedelics can change the minds of our patients. I’m hoping this research can also change the public’s and politicians’ minds about psychedelics and bring them back into medical practice, because it was absurd that they were taken from it. It’s actually the worst censorship of research and clinical practice in the history of the world. And we should rectify it now.’ DDN
The SUMH resource pack – working with people with coexisting substance use and mental health issues at www.turning-point.co.uk/reports
Gender-responsive service provision is more essential than ever at this critical point in the sector’s development, say Francesca Carpenter and Laura Ward.
Oasis Project was established in Brighton and Hove over 24 years ago by four women who felt their needs were not being met by mainstream substance misuse services. Since then, the service has vastly grown to provide a range of gender-responsive services to women, children and families affected by substance misuse across Brighton and East Sussex. Oasis is part of the commissioned structured drug and alcohol treatment delivery partnership in Brighton and Hove.
Unfortunately, women’s needs are rarely met by generic substance misuse treatment services, which are known to be male-dominated environments accessed mainly by male opiate users. For women who have experienced trauma including domestic/sexual violence perpetrated by men, male-dominated settings can be threatening and overwhelming. Whilst it is widely recognised that experience of trauma is a contributing factor in the prevalence of substance misuse across all populations, there are specific connections between women, domestic abuse and substance misuse. Women who have experienced domestic abuse are eight times more likely to develop a substance misuse problem when compared to the general population and may experience specific forms of abuse in relation to their substance misuse, such as control being exerted over their access to substances and prevention of access to support services.
Oasis’ approach includes delivery of treatment in a women-only building, providing a physically and emotionally safe place for women to access support in an environment which recognises the prevalence of trauma and actively seeks to prevent re-traumatisation and promote recovery. Women report feeling more comfortable in a setting they know is women-only, sharing space with peers and drawing on shared connections, without risk of being in groups and settings with a partner, or ex-partner.
Women who misuse drugs or alcohol are often judged more harshly by wider society than their male peers, leading to greater experiences of stigma and shame which can make accessing services more difficult. These experiences are exacerbated further still in the context of parenting, with many women fearing a disclosure of substance use will lead to separation from their children.
Services often work with either adults or with children, which can lead to age-centric thinking and approaches. The context of family at Oasis Project runs through the whole organisation and bridges gaps through wraparound family support for both parents with drug and alcohol misuse needs and children affected by familial substance misuse.
Staff are well-trained and confident in exploring children’s needs with parents and potential risks associated with substance use, and Oasis has an organisational strength around child safeguarding through our work. Our approach is to sit alongside parents to proactively reduce shame, listen to their worries and provide targeted support to reduce risks in the family including delivery of POCAR, a programme for parents whose children are in contact with social services. The relationship established with parents continues through any involvement from children’s social care, and we support parents to understand local authority processes and their rights as parents.
Childcare is a widely reported barrier for parents who need to access services, and Oasis provides a free crèche for any child affected by parental drug and alcohol use. The crèche is a therapeutic setting for children that recognises the importance of the child’s voice, views, feelings, emotions, and personality, giving every child an opportunity for space to thrive. The crèche is also a vital resource for parents, providing the opportunity to participate in activities that support their recovery, including time in the day for themselves.
Oasis provides free arts-based individual therapy for children and young people aged 5-18 years affected by a parent or family members’ substance use. This service is restorative to children who have experienced abuse and neglect in their families and seeks to provide a safe space for their own recovery. It’s important that the needs of children and young people are considered within the context of substance misuse treatment, and the families’ experience held in mind when working with parents. Parents who access Oasis Project tell us they value support being extended to their children.
It is through our specialist experience and dedication to working with women experiencing substance misuse and associated issues that we have been able to embed a responsive and trauma informed culture, practice and environment. Although necessary components, we consider gender responsive care extends beyond the provision of a women-only space, or a women’s worker, but relies upon an ethos which prioritises understanding of and responsiveness to the intersectional and specific needs and structural challenges women experience. This requires an organisational and systemic commitment to working with the root causes of addiction such as trauma, and responding through approaches which enhance safety and empowerment to promote meaningful recovery.
The promise of increased funding for treatment services through Dame Carol Black’s report and the resulting government drug strategy is really welcomed at such a critical point. Our experience has taught us that to meet the needs of women, children, and families through substance misuse treatment providers, we need gender-responsive service provision, and opportunities for joint children and adult commissioning both locally and nationally. This is essential for breaking down silos and creating greater potential for family focused approaches.
Oasis Project has recently been accredited with the One Small Thing Silver Quality Mark for working with trauma.
Francesca Carpenter is head of client services and Laura Ward is CEO of Oasis Project
Case studies
Sally’s story
Sally (24) is mum to Daniel (3). Children’s social services were involved in the family due to concerns about Sally’s alcohol use. Sally had also experienced domestic abuse from Daniel’s father before Daniel was born. Sally had been in care as a child and found social work involvement with Daniel very difficult. Sally and Daniel’s social worker referred Sally to Oasis’ POCAR programme. Sally had a dedicated keyworker, and Daniel would use the crèche whilst Sally attended appointments and groups. Sally told her keyworker she was scared that Daniel would not be able to live with her, that she had no other family support and felt lonely. Sally would drink to cope with her worries.
In POCAR Sally learnt new strategies to cope with stress and worry. Sally’s self-esteem grew which enabled her to re-connect with old friends. With support from her keyworker, Sally stopped drinking and children’s social services reduced their involvement. Sally completed POCAR and continued to use the crèche to give her opportunity to focus on her recovery. Sally is due to start therapy with Oasis to explore some of her past experiences of trauma and build resilience for future.
Taking Control
‘I’m now looking to the future and taking control of my life. It’s not been easy at all, and I have made some mistakes, but I’m learning from them. I’ve got a long way to go but I want to keep getting better and I’m willing to do whatever it takes to get there. I am slowly getting better, I’ve just got to stick at it and trust the process. I have hope which Oasis has given to me. A massive thank you to my key worker, the Oasis staff, and all the women at Oasis. I wouldn’t be where I am today without you.’ Oasis service user
Alongside adult treatment, Oasis also delivers:
Young Oasis therapeutic services to children/young people affected by a parent or family member’s substance misuse
A free crèche to provide childcare where families are accessing recovery support and parenting programmes including Mellow Parenting
POCAR, an intensive psychosocial intervention for parents whose children are in contact with social services due to risks around parental substance misuse
Tailored services for young people aged 18-25 including a Young Women’s therapy service and dedicated support to young adults new to treatment
Looking Forward, for mothers who have experienced child separation following involvement from family courts
We must be genuine in our efforts to be responsive
The number of women dying a drug-related death has increased by a staggering 80 per cent in the last decade, which is why we’re keen to support an initiative to improve women’s access to treatment (p6). We need to replace failing practice with a new system that puts women at its heart, says Karen Tyrell – well illustrated by The Oasis Project’s inspiring work (p8).
With the vast majority of people in drug and alcohol services reporting mental health problems (p10), similar giant strides are needed in developing services with an integrated approach to mental health difficulties and substance misuse. We’re still creating barriers to accessing services – ‘address your substance misuse before you can have mental health support’ – instead of accepting that there’s no neat pattern of behaviour. As the team from Bath explore (p12), most people experiencing addiction have had traumatic experiences in their lives, so we need to be genuine in our efforts to learn about and respond to this.
If there’s ever a temptation to create a service model and then expect people to fit to it, the distressing story on p16 should serve as a warning. How much time, money – and sheer anguish – could have been saved by consulting the patients as equal partners?
Most people experiencing addiction have had traumatic experiences in their lives. Trauma can cause a range of effects by disrupting a person’s sense of self, the way in which they navigate the world and the way they function. They may experience depression and anxiety and struggle to manage their emotions, build healthy relationships or trust others. People who experience trauma are at risk of developing serious mental health conditions including post-traumatic stress disorder. Using drugs and alcohol can help to numb the difficult and overwhelming symptoms related to trauma, but over time this puts these individuals at risk of addiction. Some describe substance use as a means of self-medication.
High quality drug and alcohol treatment can improve and save lives. Such treatment needs to be flexible, depending on the individual’s needs – service users should be treated with respect, listened to, receive timely mental health support, have a say in their treatment and feel safe and secure with staff from their treatment provider. This is particularly relevant for those who have had traumatic experiences, as addiction treatment may be daunting and difficult, with the potential to be retraumatising. Services should ensure risks of traumatisation are minimised – the UK clinical guidelines for drug and alcohol treatment (the ‘orange book’) advocates an approach that aims to achieve this, referred to as trauma-informed care.
Trauma-informed care is not necessarily about treating the trauma or being aware of what has happened. Instead, it’s about adopting methods and principles that acknowledge and account for the fact someone may have had traumatic experience(s). This is done by understanding the effects of trauma and the impacts it may have on people. For example, trauma could cause people to become defensive and aggressive, or they may disengage and withdraw, or have difficulties trusting the intentions of professionals.
The key principles of trauma-informed care therefore are to reduce re-traumatisation and improve treatment experience and engagement. These principles aim to create trustworthiness, safety, empowerment, choice and collaboration.
A masters project undertaken by Fleur Gill and supported by Lee Collingham, Charlotte Dack and Jenny Scott at the University of Bath interviewed 15 people with experience of using drug and alcohol treatment services. Twelve men and three women took part – the youngest was 30 and the oldest 68 with an average age of 46. Their experience of treatment services ranged from five to 30 years, with an average of 17 years, although we didn’t capture this information from five of them.
The study had the aim of understanding whether they had experiences of trauma-informed care within their treatment, and whether they felt this affected their engagement. We used the key principles of trauma-informed care to write the questions, so we could gauge if people’s accounts of their treatment experience seemed to embed a trauma-informed approach. The research also aimed to provide insight into reasons for missed appointments, which is an ongoing issue within drug and alcohol services across the UK and may be linked to a lack of trauma-informed care.
The research found that despite guideline recommendations, most people interviewed had not experienced consistent trauma-informed care. Many felt that they had had little control over their treatment, with a power imbalance between them and the service.
‘I never felt I had any power within any services. I thought they had that piece of blue paper, which was very powerful – the script.’
Many also felt that their mental health needs were not acknowledged or treated, and that their appointments lacked true purpose and meaning, with a sense of superficiality that impacted on their motivation and willingness to engage.
‘He does all that “How you feeling, how’s life” and stuff, but I think it’s just become a case of “yes, no, ok, see you next month”.’
Most participants described missing appointments through forgetting to attend, feeling too intoxicated from using or having other commitments. However, they also described feeling that the appointments weren’t important to them because of this perceived superficiality and ‘tick box’ approach.
‘Would I forget if I thought it was REALLY important? Would I still forget it?… I’ve just got to go in for five minutes say “Yeah, I’m fine” and walk out again, and it’s not gonna be much motivation for me to try and remember.’
The relationship with the professionals delivering treatment, regardless of how trauma-informed their care sounded, was important. A good relationship included feeling listened to, not being judged, feeling like they were given time, feeling empathy and for some, feeling the key worker ‘went the extra mile’. A good relationship with their key worker meant they were more likely to want to attend.
‘My last key worker, I believe if it wasn’t for her I wouldn’t be where I am today… She showed me empathy and support, but I’ve had some where they’ve felt like a bit of a number.’
However, there were consistent mentions of differences among professionals with regards to their approaches and levels of understanding. Many felt that some professionals still seem to display a lack of compassion or understanding towards addiction, despite working in the field.
‘I can remember the first time I went there he literally said, “Well just don’t use drugs” and I’m like, “You tell me how to do that then!”, cos it’s not that simple.’
Most participants mentioned how much they value staff members with lived experience, and while there is consistent evidence in published studies of the benefits of having staff with lived experience, some services are known to still adopt an approach where staff don’t disclose their experiences.
‘I’ve always found it’s when I’ve had drug workers or whatever who’ve been there and done it, who’ve got experience, they’re always better than the ones who are just textbook.’
In this study we found accounts that seemed inconsistent with trauma-informed care and we also found that positive relationships with key workers, where the client felt listened to, respected and understood, encouraged attendance. Variability among the approaches and attitudes of professionals, and their levels of understanding of addiction, was an important influence on whether the person engaged with appointments.
The benefits of staff with lived experience in supporting meaningful engagement was a key message in these interviews. By supporting more openness and honesty between staff and service users and hiring more people with lived experience, we may increase trustworthiness, safety, empowerment, choice and collaboration in treatment – key underpinning tenets of trauma-informed care.
Our study chimes with the findings of the second part of the Carol Black review, and the need for services to reorientate their approaches to enable people to engage. Finally, it’s important to say that the type of study we did is focused on understanding people’s experiences rather than generalising about the experiences of all who use drug and alcohol services. A larger study would be needed to discover if what we have found is true on a wider and more general scale.
Fleur Gill is an MSc student with an interest in addiction research; Lee Collingham is an expert by experience who supported the research project; Charlotte Dack is a lecturer at the University of Bath; Jenny Scott is a senior lecturer at the University of Bath
Three years ago, nine people in the South West of England were going about their daily lives, just as anyone else might, juggling jobs and family life with all the everyday ups and downs.
Each of them was in regular receipt of a diamorphine (heroin) script, which was working well for them in managing their dependence on opiates and giving them a good quality of life.
Then came a letter from their treatment provider – the same letter to each of them, with just their names changed. In line with ‘best practice’ they must have their treatment changed. They needed to choose a different option – oral methadone, MXL (slow-release morphine tablets), or inpatient rehab.
Four of the nine patients decided they had to challenge the decision. Jill and Helen (not their real names) talked to us about what happened and how it affected them.
‘It was clear in the letter that there was no clinical opinion taken on it,’ said Jill. ‘No individual circumstances were taken into consideration – it was done purely on a cost basis.’ She talked to the clinical lead and asked if the patients could have a meeting with the group who had made the decision, ‘to go through our opinion on it and how it was going to affect us, because nobody that made that decision had any of the rest of our personal records. I was quite concerned that the people making the decision couldn’t even put a face to me.’
Advised to put it in writing, Jill went home and wrote down the questions she needed answering. The reply around six weeks later ‘was absolute nonsense’ and didn’t clarify anything. A few more attempts later, and feeling she was being ignored, she contacted Release for advice.
Advocacy
Claire Robbins, Release’s nurse advocate and drugs advisor, explains what came next. Release wrote advocacy letters to the service provider on behalf of the patients. They introduced themselves and talked about the case, and quoted Department of Health guidance aimed at protecting patients on diamorphine. ‘It talks specifically about that group and says, if anything, their treatment should be reviewed and optimised,’ she says.
They wanted to have a conversation; there was none. The provider forwarded the letters to their litigation department and responded: ‘sorry you had to raise a complaint’. ‘We weren’t ever raising a complaint,’ says Robbins.
Release continued to advocate for Jill and Helen, but the provider refused to reconsider their decision to withdraw the medication, despite the fact that the patients had been on diamorphine for years and it having a significantly positive impact on their lives. ‘All we were trying to do was sit down and communicate with them,’ says Jill. ‘But they were not wanting to do it.’
At this stage Release involved the law firm, Leigh Day, with a view to bringing legal action against the provider.
‘We would normally advocate in a way that is respectful to all parties involved, and with the clients’ best interests and rights at the heart of the process,’ explains Robbins. ‘In the vast majority of our cases, we will resolve a problem in a positive way with the provider and the client.’ But it was not possible in this case, so Jill, Helen and the lawyers at Release decided to pursue a judicial review of the decision to withdraw medication. They did this by instructing Leigh Day.
Intimidating process
As part of the legal process, attempts were made to settle the matter. The patients tried to explain how this was affecting them – even mentioning a situation where it had happened to one of them before and led to a relapse – but felt the service wasn’t listening at all.
‘We were stressed out, really worried about it for weeks and weeks before,’ says Jill.
‘I can’t stress enough how negative this was for everybody’s mental health and the duty of care,’ says Robbins. ‘The patients were expected to go through this whole process, which was really intimidating.’
Second opinion
With no resolution and the date of the prescription change looming, the law firm took the case to court. A second opinion from an independent consultant would be sought on the provider’s clinical decision, and in the meantime the judge gave a clear instruction that the provider must do everything they could to make sure the patients’ supply was continued. It was a temporary arrangement that the organisation would have to pay for – more expense for this ‘cost-cutting’ initiative.
Then came COVID, and the temporary arrangement stretched over a year during which the provider had to continue prescribing, as the independent consultant couldn’t meet the patients. When the consultant’s decision did come, it stated that prescribing should continue.
The stress of this experience was felt physically and mentally while trying to lead as normal a life as possible. ‘I lost a lot of my hair,’ says Jill. ‘We didn’t know from one day to the next what was happening.’ But the after-effects of three and a half years of the process have had wider implications for the therapeutic relationship – or lack of it. ‘The relationship had completely broken down and the patients had lost trust,’ says Robbins.
No Support
‘We nursed each other through it – there was no one else I could talk to about it at the time, says Jill. ‘Claire was my only sanity really and I wouldn’t have done it without her. I received no calls to support me through the case from my service, only from my prescriber. He was the one that checked in on us.’
‘We had some behind-the-scenes support from workers who felt they couldn’t speak up or they would lose their jobs,’ added Helen.
Alongside demonstrating that the declared ‘best practice’ was actually very poor practice, the case cost the service a lot of money – ‘the most expensive diamorphine scripts in the world!’ says Robbins. But the outcome showed that the legal process had been essential.
‘At the core of this issue were a small number of patients who were threatened with having their long-term medication terminated without their consent, or even proper consultation,’ comments Stephen Cutter, legal services manager at Release. ‘Respect for patients’ rights must come first but when it comes to certain treatments, like diamorphine or other OST, this principle seemed to be easily set aside.
‘We wish this challenge hadn’t been needed but it does demonstrate how the law can protect the rights of people in drug treatment. Given the importance of their medication we’re relieved that these people got the help they needed, but it’s deeply frustrating it was needed at all and the process caused months of unnecessary disruption and worry to all those affected.’
Relationships are slowly being built, with help of the service’s ‘amazing’ and ‘really trustworthy’ new doctor, who is doing everything he can to tackle the latest crisis – a shortage in diamorphine supply – and is contacting pharmacies in the area to find out what stocks they have. He has assured the patients that the service will honour their prescriptions with any diamorphine they can get, and work carefully with them on titration if they need to find temporary alternatives.
Duty of Care
But the conclusion stands: that it should never have happened at all and must never be repeated.
‘The law on this matter was always clear, namely that a decision to withdraw treatment was imposed upon my clients without regard to the relevant guidance and without securing their consent or engagement,’ says Anna Dews, solicitor at Leigh Day. ‘They were owed a duty of care by their service provider and had been provided with diamorphine as an established medical treatment for many decades. I hope that the resolution of this matter means that no service provider will seek to repeat this type of decision-making in the future.’ DDN
———–
Release are UK experts on drugs and drug laws and provide advice and advocacy. A non-government and non-profit organisation, they campaign for drug policies that respect
the rights of people who use drugs.
Contact 020 7324 2989 for advice or visit release.org.uk
Lack of available data means that the ‘true extent’ of drink spiking in nightclubs and bars remains unknown, says a report from the Home Affairs Committee.
Spiking is likely to remain an ‘invisible crime’ unless more is done
The report calls for a focused approach to make sure suspected incidents are better investigated and to build up a knowledge base.
Spiking incidents include putting drugs such as GHB or prescription medications into someone’s drink, or adding more alcohol. Spiking is likely to remain an ‘invisible crime’ unless more is done to improve awareness and support victims, the document says, with issues around data collection a significant barrier to policing. The government is currently considering the creation of a new spiking criminal offence, and the committee also wants to see police forces carry out forensic testing more quickly and ‘to a quality that can be used in court’, as well as venue staff trained to identify spiking incidents.
‘There needs to be a concerted effort to stamp out spiking,’ said committee chair Dame Diana Johnson. ‘Much more work needs to be done to improve understanding and awareness so that people are reassured that the help will be there should they need it. They need to know that they will be taken seriously and action taken. It isn’t good enough to tell people to put lids on their drinks or normalise taking a testing kit out with you. Everyone should have the right to go out and enjoy themselves without fear. The message needs to be sent to perpetrators that spiking is absolutely unacceptable and will be punished.’
The charity Swanswell has completed its merger with Cranstoun, which will see the continued delivery of life-saving services and support for people to rebuild their lives.
The merger process began in 2016 and was finalised at a trustees meeting held earlier this month.
Founded in Warwickshire in 1968, Swanswell led the way in supporting recovery for vulnerable people who use alcohol and drugs and other challenges they face.
The merger is aimed at helping to grow services and world-class innovation to help people rebuild their lives in the areas of substance use and domestic abuse as well as for young people, those who need housing support and people in the criminal justice system.
Swanswell helped to develop and deliver the UK’s first diversionary Drug Education Programme in Avon & Somerset, helping people who use drugs entering the criminal justice system address the underlying causes of their addiction.
Leading ideas like this have continued since the beginning of the merger with Cranstoun, with the launch of education programmes like DIVERT and the Cranstoun Arrest Referral Service operated in the West Midlands.
Cranstoun has over 450 employees working across England to deliver services.
Charlie Mack, Chief Executive at Cranstoun, said, “The wealth of knowledge and experience that the team from Swanswell have brought across to Cranstoun over the past six years has been invaluable.
“Our shared values made the merging of the charities easier. We are committed to our vision to innovate and continue developing world-class services.”
Andy Furlong, who served as Swanswell’s final Chair of Trustees, oversaw the smooth wind-down and closure of the charity’s head office in Rugby. He has now joined the Cranstoun board. He added:
“Together, Swanswell and Cranstoun have over a century’s experience in providing support for some of the most vulnerable people in society.
“By merging, we will be able to do more to innovate and improve delivery for the people who use our services across the country.
“We are proud of our history but filled with excitement for the future. With a new, ambitious strategy guiding us for the coming years, the skills and experiences we have brought together through the merger will help us grow our reach and increase our services.”
US president Joe Biden has sent his administration’s first National drug control strategy to Congress, focusing on a whole-government approach to the country’s ‘overdose epidemic’. Almost 107,000 people in the US died a drug-related death in the 12-month period to November 2021.
The strategy is the first to ‘champion harm reduction to meet people where they are and engage them in care and services’, the White House states, as interventions like naloxone and NSP are often still restricted or underfunded at community level. Less than 7 per cent of the 41m people needing treatment for substance issues were able to access it, according to the 2020 national survey on drug use and health.
President Joe Biden: a whole-government approach to the ‘overdose epidemic’
The strategy calls for more access to harm reduction interventions like naloxone, NSP and fentanyl test strips, and directs federal agencies to integrate them into care systems. Naloxone, however, will remain prescription only and will not be available over the counter. The administration’s efforts to expand access to treatment will focus on high-risk populations like people experiencing homelessness and people in – or leaving – prison. ‘The Biden-Harris Administration is committed to deploying an evidence-based approach to policy making,’ the White House says, combined with a focus on addressing trafficking and supply. The administration has submitted budget requests for an extra $300m each for the Drug Enforcement Administration (DEA) and Customs and Border Protection (CBP).
Existing harm reduction policies were ‘failing people’ as a result of inconsistency and barriers to access, director of the White House Office of National Drug Control Policy, Dr Rahul Gupta, told CNN. ‘We’re failing to meet them where they are and every one of those overdoses – from an opioids perspective – is reversible. Your zip code defines whether you live or die and that should just not happen. President Biden has made sure that this is an urgent priority, and we need to act with a sense of urgency because this is not a matter of days, weeks or years. It’s a matter of every minute when we lose Americans.’
‘We applaud the Biden-Harris Administration for taking the historic step to support access and funding for harm reduction services and reduce barriers to life-saving medications,’ said Grant Smith of the Drug Policy Alliance NGO. ‘Despite over 1m lives lost to drug overdose over the last 20-plus years, this is the first time an administration has included harm reduction in the National drug control strategy. The administration should continue to focus on its promise of equity by decreasing racial disparities in drug policy and the overdose crisis. Criminalisation approaches only saddle mostly Black, Hispanic and Indigenous people with criminal legal records and often incarceration, which increases their risk for infectious diseases, overdose and death.’
Prioritising spending on public health rather than enforcement was the best path forward, he stated. With the overdose crisis ‘now costing the US economy over $1tn annually we must embrace the evidence-based public health approaches we know work and save lives. But it must be done outside of the harmful apparatus of the drug war to be effective and provide the kind of racial equity this administration has long promised.’
GambleAware is investing £2.5m in gambling education programmes across England and Wales, the charity has announced.
Young people are ‘increasingly exposed to easily accessible gambling’ via social media and online gaming.
The money will go to GamCare, YGAM and Adferiad Recovery to expand the Gambling Education Hub programmes, which include toolkits, training and peer-based drama performances aimed at professionals and volunteers. The investment is part of the charity’s commitment to ‘help reduce gambling harms among young people’, it says.
The Gambling Education Hub uses early intervention and prevention methods to reduce gambling harms among children and young people, and incorporates input from people with lived experience of gambling harms. An independent audit of the Scottish Gambling Education Hub – which delivered education and training to almost 3,000 professionals and volunteers, as well as parents, carers and young people themselves – found that more than 90 per cent of practitioners and youth workers felt confident in identifying signs of gambling harm among young people, compared to 35 per cent pre-training.
Research by the charity revealed that almost 95 per cent of 11 to 17-year-olds had been exposed to gambling advertising in the previous month, seeing around six adverts on average, with young people ‘increasingly exposed to easily accessible gambling’ via social media and online gaming.
‘At a time when young people are increasingly exposed to gambling, the delivery of local focused programmes for gambling education and prevention of harms has never been more important,’ said GambleAware chief executive Zoë Osmond. ‘We hope to see the positive short-term impacts from the Scottish Education Hub’s activities replicated in our newly commissioned English and Welsh education hubs, and we are excited to have awarded this grant to these two highly experienced organisations. With young people in the UK now growing up being widely exposed to gambling marketing and advertising, these projects represent a meaningful step towards delivering a society where all children and young people are protected from the risks of gambling-related harms.’
Meanwhile, new NICE guidance to support the safe prescribing of medicines such as opioids, benzodiazepines and gabapentinoids has been criticised by the APPG for Prescribed Drug Dependence for failing to provide simple instructions for slow tapering, the ‘most important intervention for safe withdrawal’. Without this doctors are unlikely to change their current practice, the APPG states, with many patients being taken off drugs too quickly and reporting ‘devastating’ withdrawal symptoms.
’It is very disappointing that these new guidelines fail to include the simple instructions for slow tapering which are desperately needed by doctors to support safe withdrawal from these drugs,’ said APPG chair Danny Kruger. ‘This is because important evidence developed with patient groups has been ignored, as it doesn’t meet NICE quality standards. We will be urging NICE to reconsider both this evidence and their process to ensure that patient experience is properly represented in future.’
Medicines associated with dependence or withdrawal symptoms: safe prescribing and withdrawal management for adults at www.nice.org.uk/guidance/NG215
Religion and psychology are often seen as separate or potentially opposing, but I don’t see it that way, writes With You’s Rodean Vafa.
I’m a Cognitive Behavioural Therapist with 10 years’ experience, working for With You in Kent and Surrey’s Improving Access to Psychological Therapies (IAPT) service. Our service offers free therapeutic support for common mental health difficulties to adults in Kent and Surrey. As someone who identifies as male, and comes from a cultural background with a Muslim majority demographic, I represent a minority demographic of therapists in the UK.
Mental health problems affect everyone, regardless of their race, religion or other cultural backgrounds. That said, historically, people from certain religious communities are underrepresented in IAPT therapy services across the UK. National IAPT data shows that while Muslims made up 5% of the population of England and Wales in 2011, only 2% of those accessing IAPT services are Muslim.
I don’t believe that this means people from these backgrounds are less likely to seek help for mental health issues. Instead, they are more likely to seek help from cultural resources that they are more familiar with. For example, a practising Muslim may be more likely to try to improve their mental health through faith and religious guidance for a number of reasons.
One of these reasons is they might feel that mental health therapy services are not suited to them. In many ways, I feel I can personally understand why public therapy services may not seem like a viable option for certain people in this community. If you don’t see yourself reflected in the service’s workforce, you may feel that staff wouldn’t be able to understand your cultural situation.
According to the IAPT 2020 national census, approximately 86% of all staff is White-British, with Black, Asian and other underrepresented demographics only representing approximately 14% of the total workforce. In this case, a practicing Muslim person may be more likely to seek support from someone who has knowledge of Islam over an expert in mental health. This is something our organisation has recognised, not only internally but across health services in the UK.
To help address this, With You in Kent & Surrey created my role, Equality, Diversity and Inclusion lead, to work on how we better engage with underrepresented communities, with a focus on our local Muslim community. An example of this effort has been the creation of an inclusive calendar to recognise and observe dates not included in the shared British calendar. This helped our team to be aware of important dates like the start of Ramadan and Eid al-Fitr. By being aware of these dates, we can make adjustments for staff and the people we support. We’re also developing a training workshop for our staff to share knowledge about Islamic values and outreach materials to help us share what we do more effectively with our local Muslim communities.
Religion and psychology are often seen as separate or potentially opposing, but I don’t see it that way. There are several Islamic concepts which deal with mental health that I find to be quite similar to concepts in psychology. For example, the Islamic concept of ‘tawakul’ refers to giving over control to God on things that are out of our hands. A similar concept is also found in cognitive behavioural therapy (CBT) called ‘tolerating uncertainty’, and is fundamental to the understanding of why people suffer from anxiety. In both Islam and CBT the guidance is to try to let go of habits such as over-worrying to help deal with anxiety.
Islam also has contributed much to the development of psychology. The world’s first mental health hospital and psychiatric ward were constructed in Baghdad, Iraq by Abu Bakar Muhammad Zakaria Al-Razi in 705CE. Seeking help for mental health difficulties is also widely accepted and encouraged by Islamic scholars. The Quran mentions Allah (SWT) creating treatments for difficulties and illness:
“So, verily, with every difficulty, there is relief: Verily, with every difficulty there is relief.” (Quran, 94: 5–6)
Fifty of England’s most deprived areas are to receive ‘significantly more’ funding in 2022-23 to bolster their drug and alcohol treatment services, says the Department of Health and Social Care (DHSC).
While all local authorities will receive additional funding as part of the government’s three-year £780m investment in treatment announced late last year, those areas ‘most affected by drug-related crime and addiction’ – including Birmingham, County Durham and Leeds – will receive additional funding totalling £300m over the three year period.
The money will help to improve access to treatment and increase the capacity of services, said health secretary Sajid Javid. ‘This is a significant step in our commitment to rebuild the drug treatment system, save lives and level up the country,’ he stated. ‘We’re investing a record amount in treatment services and ensuring some of the most deprived areas in England are first in line for this funding. Treatment is just one element of our far-reaching strategy to better rehabilitate drug users – whether it’s helping people get jobs, creating a stable home or cracking down on supply.’
The money will help to improve access to treatment, said health secretary Sajid Javid
The government has also announced plans to enhance its Project ADDER scheme through ‘more intensive oversight’ by the criminal justice system. A support package will be provided to all opiate and crack users in ADDER areas, it says, while people who commit ‘neighbourhood crimes’ like burglary, robbery or theft will be subject to ‘joint probation and police supervision’, with more frequent contact from the authorities and improved information sharing between agencies. The plans will also see greater use of community sentences with drug rehabilitation requirements, drug testing and ‘stronger electronic monitoring options’, the government states.
‘The rate of drug-related deaths remains at crisis levels and each death sends ripples through families and communities, with the impact continuing to be felt years down the line,’ commented Jon Murray, With You Director of Services for England. ‘It’s important to remember that problematic drug use is often a reaction to people’s surroundings,’ he said. ‘Issues such as rising homelessness, poor mental health and a lack of economic opportunities in some areas can all lead to people using drugs. With this in mind, there’s no surprise that drug related deaths are highest in the country’s most deprived areas.
‘Each area faces their own distinct and complex challenges but what we can already say is that further funding could be used to increase the number of people who can access treatment, contribute to wider provision of naloxone as well as improving workforce skills.’
His charity welcomed the ‘serious political commitment to investing in treatment’ and looked forward to ‘working collaboratively to address these complex issues, with the compassion and support people deserve’.
‘One of the questions I often get asked is why Middlesbrough, and why now?’ said Daniel Ahmed,clinical partner at specialist GP practice Foundations and who runs England’s only diamorphine treatment programme in Middlesbrough (DDN, December 2020/January 2021, page 4).
‘We’ve got a perfect storm.’ Not only was Middlesbrough the most deprived local authority in England, it also had the country’s highest number of heroin users per head of population and high rates of drug-related deaths.
Daniel Ahmed (right) and the Cleveland police and crime commissioner Barry Coppinger launched the UK’s first heroin assisted treatment pilot in Middleborough, in 2019. Credit: PA Images.
The average age of patients at Foundations was 38, he said, ‘so a relatively young group of people. But their prevalence of significant health conditions is staggeringly increased compared to the national average. We’re looking at medieval levels of life expectancy within this patient population, which is why we need to be exploring all the available treatment options to support the complex needs of this group.’
In preparation for the diamorphine-assisted treatment programme, he and his colleagues had looked at around 20 people who had been ‘caught in a cycle of failure to benefit from treatment’, sometimes for decades. Managing the group through the criminal justice system alone cost around £2m, he said – a cost that ‘wasn’t improving the outcomes of anyone involved’.
All of this meant there was an argument for addressing their needs in a different way, and there was strong evidence that supervised diamorphine as a second-line medication for people failing to benefit from treatment was highly effective. The principle was the same as in any other area of medicine, he said. ‘If you’re treating someone with an antibiotic and it fails to benefit, you might change it for one that’s a bit stronger and more targeted.’
The team began a programme of engagement with the public and media to share the evidence and explain why the intervention was needed. ‘It was relatively successful, although the Daily Mail approached a number of our neighbours and suggested we were giving away free heroin.’ In fact, a key early mistake had been use of the word ‘heroin’, he said. ‘It has connotations for the public, other professionals and patients, so we’ve moved to “diamorphine-assisted treatment”.’
Funding was initially secured to treat 20 people, with the programme going live in October 2019. People turn up twice a day, seven days a week, requiring a huge level of commitment, he said, and the service was currently funded for ten people. ‘Their drug use is stable, and their treatment concordance is excellent.’ However, the clinic was still in discussions around what level of funding it would receive to continue the work. ‘This is where we’re coming across some interesting attitudes in senior public health figures. I think there are some really ingrained negative perceptions about the programme, and the argument that all treatment interventions need to be targeted at a large population.’
The programme was under constant independent evaluation, he said, ‘and we have no problem with that because it just adds to the body of evidence.’ Research by Teesside University found that some people were stabilising more quickly than expected and soon asking to be moved from two to one dose a day, with some successfully finishing treatment. ‘They’re completely drug-free and looking at being an ambassador for the wider treatment system.’
There had been no drug-related deaths among anyone engaged in the programme, with the majority now abstinent from street heroin. ‘Some individuals may slip up, but in terms of their overall level of heroin use it’s a dramatic reduction, and there’s been significant reduction in harm.’ People who had been regularly visiting hospital for wounds and infections were no longer attending, and clients had reduced their overall consumption of other substances. There was also 100 per cent engagement in non-mandatory psychosocial interventions by month ten.
‘There’s been a dramatic improvement in physical and psychological health, and a real increase in everybody’s social stability,’ he said. People who were street homeless had managed to get into secure housing, with those in supported accommodation able to move to independent living. There was also a 60 per cent reduction in both criminal behaviour and its severity, he said. ‘But we’re pushing for research into savings to the wider economy because we think they’re far greater.’
In terms of other areas launching similar programmes, ‘I think the appetite is there,’ he said. ‘I know services that want to get involved.’ There was resistance, however, mainly from the public health argument that only a small number of people were impacted. ‘But that forgets that by targeting a particular group it’s been shown to be cost-effective. I think it’s about us as a sector shouting that this is an evidence-based intervention. We’re talking about world-class treatment, so why haven’t we got this available for anybody who needs it?’
Dr David Bremner is group medical director at Turning Point
A Delicate balance
While the will to offer diamorphine is there, a crisis in supply makes for difficult choices says Dr David Bremner.
The diamorphine shortage is not a conspiracy but a very real concern, with patients increasingly unable to get their prescriptions filled as and when they are needed.
Despite what some advocates, pharmacies, manufacturers and distributors might say about supposed stock levels, prescribing processes dictate that promises of plenty do not always result in medication in hand. And when prescriptions can’t be filled, patients face undue risks, something my team and I always aim to avoid.
As an organisation, Turning Point are quick to use depot buprenorphine injections – cost does not dictate. The limited numbers of people on diamorphine is not a significant cost burden to my organisation, which has never challenged me or my formulary for including it. But supply is unreliable.
It is hard to swap out diamorphine in an emergency and therefore getting harder and harder to justify prescribing it. As many of the recipients tell me, not having prescribed diamorphine is a strong push back to ever more toxic street heroin.
Supply disruption is well documented – medicines supply notifications, supply disruption permanent actions, clear legislation around use of split dosing and finally, the cessation of production of 500mg ampoules. There are few 5mg and 10mg ampoules, over utilised 30mg and 100mg ampoules and no more 500mg ampoules.
Advice to swap to something more readily available has been met with ‘I will take my chances’ from most recipients, but what are we letting people take their chances with?
The second shortage of 2021 was sudden, hours before a bank holiday, making re-titration onto alternatives tricky and slow. Some swapped medications, getting a generic methadone conversion that holidays and pharmacy opening hours permitted, some went without. Travel plans and family occasions were impacted. We managed but this should have been done electively and in a planned way.
What is the clinician’s role in this? Should we keep prescribing a drug that faces multiple shortages a year when the emergency provision for an alternative has proven to be so inadequate and the consequences, as foretold by the patient, are threatened to be fatal? Or do we not allow people to ‘take their chances’ and undergo a safer elective swap in medication while trampling on patient choice?
This is our sometime rock and hard place, the constant balance of patient safety and patient choice.
Individual Placement and Support (IPS) can have a hugely positive impact for people with experience of addiction, says Rebecca Odedra.
Paid employment plays such a huge part in so many people’s lives. It provides a reason to get out of bed in the morning; it can boost confidence, motivation, empowerment, financial independence, increased social networks, and so much more.
For a lot of people, work can take up more than 60 per cent of their waking hours, so it’s no wonder that – as a survey quoted in Dame Carol Black’s 2016 independent review into the impact on employment outcomes of drug or alcohol addiction, and obesity said – ‘getting a job (and keeping a job) is a top objective for people in treatment, only second to “getting clean”’. Our experience at WDP also tells us that employment is vital to people’s recovery with improved drug and alcohol treatment outcomes – including reductions in the frequency and severity of relapses.
In 2019, we were awarded an Individual Placement and Support (IPS) contract through West London Alliance to work across eight West London boroughs. IPS Into Work is an intensive and personalised service provided by expert employment specialists who understand the ebbs and flows of recovery. Focussing on client readiness to enter work, a rapid job search, and working with employers, our award-winning team is dynamic and innovative but perhaps most importantly, believes that anyone that wants to work can work.
As featured in our recent impact report, we’re proud to have supported over 250 employment outcomes, provided more than 4,000 hours of support, and that 100 per cent of participants recommend the programme.
The impact of work is hugely significant and truly transformative, and so many of our clients’ stories have stuck with me. I recall one individual we helped who had not worked in over 40 years. Getting that job was life changing – enabling them to have an improved relationship with their child and creating structure and financial independence.
Another testament to our success is having recently received additional funding from the Department for Work and Pensions (DWP), supported by the Department of Health and Social Care (DHSC), to extend our existing contract and expand into a ninth London borough, Hammersmith and Fulham.
Rebecca accepts the Transforming Lives Achievement Award at the 2021 MJ Awards. The awards celebrate the delivery of services and showcase their role in communities across the UK.
With the recent drug strategy announcement committing to roll out IPS in every local authority by 2025, the future looks very promising in the world of IPS and for those individuals it can help. But don’t take my word for it, hear from two people who have experienced the power of IPS.
The IPS model impressed the judges who said it was not only changing perceptions of drug and alcohol problems but also empowering people through a cross-partnering approach. See more here.
Rebecca Odedra is head of reintegration at WDP
———-
In the right place – Brian’s story
I had been in custody serving a mandatory life sentence and was released on parole [after 17 years].
My work background before I went to prison was mainly machine driving, but also building and construction, warehouse jobs and driving jobs. I’ve had spells off from time to time due to factors going on in my life, whether it be drink, drugs, family issues, poor emotional management, or not being able to cope properly. But I’ve always worked, and I’ve always managed to get myself a job and have a bit of stability.
When I first got released, I found [job searching] a bit difficult because they wanted CVs and disclosure letters, which I had but at that time I needed to get them updated and readdress how to put it together in a professional manner.
Before I went to prison, I would just phone up an employer, get an ad out of the newspaper, or pop into the Jobcentre to look at their list. And that was gone, and everything was just email. And because of COVID, you couldn’t have in-person conversations with people.
[Having moved to a new area] I ended up working with WDP initially through drugs and alcohol prevention, but they said they could help me with finding employment as well.
In my first meeting with my employment specialist, we managed to get an understanding of one another, and I got the help I was looking for. They talked about a couple of possible jobs they found, and we sent my CV off. And lo and behold, I got the email from one of the companies saying they’d like to invite me to a day down at the company. It sort of took off from there and I ended up getting the job.
The job that I got was a collection driver for a waste recycling company and I’m loving it. I like driving and being out on the road because it’s helping me to get to know my way around again and meeting new people and dealing with customers, and I enjoy that type of work. My main focus now is to settle into the job that I’m in and I’m also hoping to do HGV training to just keep bettering myself as I go along.
I’d rather tell the people that I’m working for about my history because that then gives them a better understanding of me, my life, what’s happened in the past, and that I’m just trying to rebuild my life. It gives us more trust. That’s why I’d rather be open and honest at the beginning to give them that option to say, ‘Sorry we can’t employ you’ or ‘We’re willing to give you a second chance’. We all make mistakes, and a lot of people understand. And I’m grateful for that.
———-
Tailored support – Leo’s story
I didn’t pick up my first drink until the age of 20 but from that point, I drank very heavily. In the mid-1990s, cocaine became part of my story as well and the consequences started to kick in.
By 2000, I was completely out of control, barely hanging on to my job, and I went to the first of six treatment centres. When I left, I should have gone to a ‘dry house’, but I chose not to – I wanted to return to work. I returned to work five weeks after leaving and relapsed within a week. By 2001, my employer said, ‘We need to part company with you’.
In 2002, I sold a property for quite a sum of money. But if you’ve got a cocaine habit of at least one or two grams a day and you’re drinking, buying holidays, sports cars, that type of thing – by 2008, the money had gone. From then until a year and half ago, I started to claim benefits and was doing odd jobs, manual jobs, gardening.
I was very fortunate as I ended up engaged with a treatment service (now WDP) and a housing officer found me a secure roof over my head. But up until a year and a half ago, I had become a hermit. I didn’t engage with life, with people, and I wasn’t in a good place. I was so lonely, worried, and fearful, and I didn’t know what was going to happen.
But things changed infinitely for the better 18 months ago. I had tried to commit suicide but was lucky – I woke up, I escaped, I got away with it. I then reconnected with WDP and was also referred to the IPS service.
My employment specialist carried out a detailed assessment and really got to know me. He wanted to know my journey and understand what my needs were. He then put together a tailored support package. He was very helpful with my CV as there were some significant gaps which we jointly addressed. He would send through jobs every week based on what I wanted, which was a customer service position.
One job was with a US corporate hospitality and food company, and I had to answer some questions by video. They said they were very happy with my interview and offered me a job. I am now working there and about to start another job as an events steward. My focus for this year is working for these two companies and then I’ll start to think about what’s next.
IPS has been an extraordinarily supportive tool to me returning to normality. It builds your self-esteem, your self-worth, and it provides structure and socialisation once you are back in work. I am very grateful and couldn’t commend them more highly.
Phoenix Futures recently launched a report looking at the state of residential treatment provision in England. Through a series of blogs and articles, Phoenix continues to explore the theme of Making Rehab Work.
The experiences of people involved with substances, crime and the justice system are complicated. Drug offences accounted for 16% of all prison sentences in the UK in 2021 and this figure does not account for the number of violent or acquisitive crimes where substances were involved. There is also growing concern for people exposed to substances during a custodial sentence, with UK government statistics showing that between 2014 and 2019 the proportion of people who developed a drug problem whilst in custody doubled from 8% to 15%.
At Phoenix Futures, our residential treatment services welcome residents directly from prison and many more who have had lived experience of the justice system in their past. To even talk about crime can feed into a stigmatising narrative that some people in society use against our residents, and so some of our current residents were kind enough to share their personal experiences to help us explore these complex issues.
Chelsea began taking drugs at 15, and by age 19 had received her first prison sentence. The following twenty years she described as a ‘revolving door’, only staying out of prison for a few months at a time before returning. She spoke of the complicated relationship she had with prison.
“Sometimes it was a relief to go back,” she said, “because I couldn’t get to rehab, I treated prison like a rehab. I knew I could get drugs in there if I wanted to, but I never chased it. I was actually clean when I was in there, I did well. Whenever I came out, my life was chaos.”
When asked whether prison had helped prepare Chelsea for rehab in any way, she was keen to emphasise the vast difference between the two settings.
“I thrived on the structure, the routine, the discipline in jail but in there nothing is expected of you. It’s not like being in rehab, where from the moment you wake up you have to think about how you feel and how you act.
“In jail, you have to put up a front and not let your guard down in order to protect yourself.”
Kelly too had a similar experience, using heroin at 14 and continuing until the day her son was born. Her first prison sentence came at age 17, and a further thirteen periods of imprisonment followed.
“In prison, I had walls and defences up. I wouldn’t stop and think,” she said. “In there you’re surrounded by people who don’t want to change. I wasn’t happy in that life, but you end up just accepting it.”
Many of the behaviours Kelly had adopted in prison were carried into her life after release, and despite her desire to access rehab with her son, it took some time for her to adjust.
“When I first came to rehab, I would kick off straight away if I didn’t like the answers from staff, I couldn’t keep my mouth shut,” she said. “But once you’ve built the trust, it is massive. In here you’re encouraged to change and challenge your behaviours, and you don’t realise they change until its done.”
Kelly continued, reflecting on how fortunate she felt that help was there at the right time in her life.
“Without my son I’d still be on the same path, using and going in and out of prison. Time is big, you don’t realise it’s running out. If I could do it over again, I would have surrounded myself with people who were better for me.”
Peers in Medway are taking partnerships to a new level with impressive results. DDN sees them in action.
Read it in DDN Magazine
A man in a grey tracksuit wanders around Chatham High Street, duffle bag in one hand, drink can in the other. He’s newly released from prison with nowhere to head and no real plan.
Jenna and Sam spot him and head over with a casual ‘how’s it going?’ They’re peer workers at Medway Hope – part of Open Road’s support and recovery network in partnership with Turning Point – and within minutes they’ve established that he needs meds as well as somewhere to stay. A quick phone call and he’s booked in for a prescription and linked to local services. He seems surprised – and grateful to be in the right place at the right time.
For Jenna and Sam – and their peers at Medway Hope – this is always a good place, and using their Red Card scheme makes it easier for it to be the right time. The scheme represents a hotline to services, meaning they can call a colleague and arrange a fast-track appointment for someone they come across who is ready for help. It opens the door to services and makes it much easier for someone to walk through it.
The team brandish naloxone kits when they’re out and about – a conversation starter as well as a vital harm reduction intervention. They wear their naloxone shirts and are proud to spread the word as Medway naloxone peers. On their route down the high street they stop to talk to two young men who are willing to hear more and engage in answering some questions – ‘What are the main causes of an overdose? When are the high-risk times? What are the signs and symptoms of an overdose? What should you not do in an overdose situation…?’ The men carry on their way with naloxone kits and the knowledge and confidence to use them, saying they ‘learned something very useful’.
But the peers’ work is not just about giving out kits. ‘I target anybody and everybody that’ll listen to me,’ says Sam. ‘It’s about throwing myself in the deep end, saying you might not use drugs yourself but be around someone who does. It’s generally well received.’
Stepping through a modest door on the high street offers up a warm welcome at Open Road, with comfy chairs, coffee and cheerful chatter. Art adorns the walls and it’s a bright and creative space. Today the Medway Hope naloxone champion steering group has assembled – peers, commissioners and colleagues from the providers, Turning Point and Open Road, who work closely together to offer drug and alcohol services and recovery support. The forum is also regularly attended by representatives from police and the local council, who link with the many services across immigration, community safety, housing and health. George Charlton – consultant, trainer and ‘Naloxone Man’, who has been supporting the peers – has come down from the North East and all the participants are ‘buzzing’ to see each other.
As they work through an agenda that covers their progress over the last few months they realise their partnership working is paying off and results are tangible – for clients and for the team members themselves. The growth and development of the peer group is an important part of this story.
From tentative beginnings and with a lot of encouragement and (justified) positive feedback, the peers have gone from strength to strength and grown in confidence. The Open Road PREMIER Award takes pride of place in the reception area and they explain that it’s the first time that a project, rather than a service, has won it – all achieved in six months. ‘You’re leading the way, cutting your own path,’ George tells them. ‘People are here today because of your interventions.
Everyone seems motivated by the momentum and keen to grow the partnership. Commissioner Claire Hurcum has been a key facilitator, and says she is proud of what the team of five peers have achieved together in six months. ‘I can see the growth in all of you. As commissioners we’re really pleased – you should be really proud of yourselves,’ she tells them. She hoped there would be further expansion of the team’s work, and that it would lead to them becoming a peer-led support network. With George’s encouragement, the group went on to discuss next steps and aspirations – perhaps they could become a lived experience recovery organisation (LERO) or develop a community interest company (CIC). The team dynamic felt full of possibilities.
The staff team (clockwise TL): Aaron, Jo Payne, Claire Hurcum, Svajune Ulinskiene
The steering group ran smoothly and it was full of positivity and great feedback. But it’s clear that a lot of hard work has happened – at a fast pace – to create this environment, and a determination to share the vision, particularly with so many partners on board. ‘We’re all just people with a common goal – to move things forward,’ said George after the meeting. ‘You hear talk of drug users as hidden populations, but they’re not – it could be providers who are hidden in buildings. Peers are the first people to see trends.’
The team had built skills around naloxone ‘because of the immediacy’, but a whole raft of harm reduction initiatives had followed swiftly within six months – training with needle and syringe programmes, sexual health advice and condoms, dry blood spot testing and dealing with drugs litter. ‘It’s really action orientated… we slice straight though,’ he said, adding that much depended on ‘the need to get our heads out of bureaucracy and do some straight talking, recognising the strengths of both parties. Then the provider becomes a real asset.’
Svajune Ulinskiene, service manager at Turning Point, agreed that ‘we’re trying to achieve the same goal’ and always sought to be inclusive. Peers were a vital part of understanding the needs of the area, she said and had told them at the meeting, ‘the knowledge you bring is amazing’. Doing a care plan meant working with lots of different services, not just substance misuse, to look at what recovery was about for the individual. Assessing and adjusting how services operated involved talking to the peers and then thinking about the evidence.
While Turning Point had always worked with peers, COVID had led them to work in a different way, she said: ‘Before, we were risk averse, but we had to change and act quickly. It changed the clinicians’ thinking.’ They needed to listen, respond and work closely together to make sure help reached those who depended on it.
Jo Payne, volunteer and building recovery coordinator, has worked with Open Road since 2018 and has seen the peer support develop as the partnerships have evolved. The peer projects now reach into all areas of work – outreach, naloxone, sexual health, the hep C clinic, rough sleeper initiatives with the council, the Ladies’ Night project with sex workers. With 24 peer mentors, ‘it’s known as a safe place to be,’ she says. Furthermore, ‘peer mentor support has become integral to services’ and peer mentors regularly work at Turning Point, co-facilitating groups.
It’s also given the capacity to develop partnerships to integrate into communities, she explains, with relapse prevention groups, and diversionary projects such as allotments, art and mindfulness. The walls of their space at Open Road are covered in paintings and a community arts exhibition is being planned for July. ‘We’re known for the social side here,’ she says.
Leaving the building with a group of peers proves the point, as Brian advances on the group, all hugs and smiles. His desperate years of alcohol, fighting and prison are behind him, he says. Through embarking on college courses he was put in touch with Open Road, and his life changed. He found the support he needed, discovered love and happiness, and ‘never looked back’. ‘It’s nice to be on the giving end,’ he says, heading into the service to play his part. And so the network keeps growing and flourishing, stronger for the experience of every member.
SIG’s Synergy office has been visited by Sarah Owen, Luton MP and Shadow Minister for Homelessness, Rough Sleeping and Faith.
The visit introduced Ms Owen to the Synergy Universal Service, which carries out vital work in the community, including working with families experiencing or at risk of homelessness.
Emmeline Irvine, SIG’s Head of Complex Needs and Homelessness, hosted Ms Owen, who toured the building, met the SIG Penrose Synergy universal team, and held discussions with staff. Discussions centred on funding for families experiencing homelessness and working together to support other areas of local need. Safeguarding the vulnerable and safe spaces for victims of domestic abuse, including Penrose’s specialist women’s outreach project CATE funded by the Bedfordshire Police and Crime Commissioner, was also discussed.
Ms Own was given an overview of the additional support services offered by Synergy, including MHFS, STEPS and Bridge House, which supports women and children.
“We are grateful to Ms Owen for her visit and openness to discuss Synergy’s vital work in the community. We hope to work together to highlight the need for better funding for those most vulnerable,” said Emmeline.
Ms Owen’s visit is part of SIG’s strategic partnership working model which aims to form stronger alliances with partners and agencies to allow for greater collaboration and efficiency.
Ms Owen said: “It was wonderful to spend time with the dedicated team at SIG Penrose. Hearing about their brilliant work first-hand, it is clear they are vital to hundreds of vulnerable people, families and especially those fleeing domestic abuse. SIG Penrose not only helps with housing, but they support a person’s needs as a whole – from their mental health to welfare support and much more. I look forward to continuing working with SIG Penrose for the good of our town and to support people through these challenging times.”
Well done to Emmeline and the team at Synergy for the effort they put into arranging and hosting the visit.
Gambling and lottery advertising will no longer be able to use content ‘likely to be of strong appeal to children or young persons’, the Committee for Advertising Practice (CAP) has announced, especially that associated with youth culture. This means that prominent sports personalities, celebrities and social media influencers will no longer be able promote gambling brands if they strongly appeal to those under 18.
The restrictions, which will come into force in October, include ‘all sportspeople well-known to under-18s’ – including topflight footballers and those with large social media followings – as well as people from reality TV shows popular with young people, and any references to video game content.
Shahriar Coupal: A ‘new era’ for gambling advertising
The announcement follows a wide-ranging consultation by CAP launched partly in response to research by GambleAware which found that even advertising abiding by the existing codes had ‘more potential than previously understood’ to adversely affect children or vulnerable people (DDN, November 2020, page 5). The All-Party Parliamentary Group (APPG) for Gambling Related Harm has previously called for all gambling advertising to be banned.
‘The days of gambling ads featuring sports stars, video game imagery and other content of strong appeal to under-18s are numbered,’ said CAP director Shahriar Coupal. ‘By ending these practices, our new rules invite a new era for gambling ads, more particular to the adult audience they can target and more befitting of the age-restricted product they’re promoting.’
Grant Shapps: No room to be lax on drug driving
Meanwhile, the Department for Transport (DfT) has launched a call for evidence on whether people convicted of drug-driving should be required to undertake rehabilitation courses before being allowed to drive again. While deaths and injuries related to drink driving are now ‘very rare’ in the UK, says DfT, more than 700 people were seriously injured in drug-driving collisions in 2020, up from under 500 in 2016.
‘Drink-driving is now rightly seen as a social taboo by most of us in this country and we have worked hard to drive down drink-drive related deaths,’ said transport secretary Grant Shapps. ‘But if we are to make our roads safer still there is no room to be lax on drug-driving, which is why I have launched this call for evidence today. It’s only right that drug-drivers must undergo rehabilitation before getting back behind the wheel, helping protect the public from this hidden problem and stamping out drug-driving for good.’
The time was long overdue for looking at alternatives to a criminal justice-based approach to drugs, heard delegates at the Royal College of GPs and Addiction Professionals online conference.
‘We’d all much prefer to be wise before the event,’ chair of the Independent Advisory Panel on Deaths in Custody (IAPDC), Juliet Lyon, told the Managing drug and alcohol problems in primary care conference. When it came to reducing drug-related deaths in custody settings there ‘could be a much greater use of harm reduction initiatives, and a much better dissemination of recommendations’ following a death – ‘to learn what could have been done and apply that’.
Her panel – which advises the Home Office, DHSC and the Ministry of Justice – had recently produced a report concluding that it was vital to take a whole-systems approach to deaths in custody (www.drinkanddrugsnews.com/whole-system-approach-needed-to-tackle-prison-drug-deaths). There needed to be a better database for understanding the extent of the problem, as well as improved court-based liaison and diversion services when it came to sentencing. While community sentences with treatment requirements had been on the statute book for decades they remained ‘spectacularly under-used’, she said. There was a problem in terms of both magistrates’ confidence around them and availability. Magistrates ‘would say these things aren’t available in our area or we simply don’t have enough information. It’s a terrifically wasted opportunity.’
Context
A letter from a prisoner had pointed out that any attempt to tackle alcohol and drug-related deaths in custody would need to address ‘many aspects’ of prison life. ‘It’s the overall context in which people are living, and of course this has been exacerbated massively by COVID. The kind of desperation we’ve been seeing, the crushing boredom, living 23 hours a day in a six-by-nine cell often shared with a stranger.’ It was clear why people would turn to ‘any substance’ to try to block this out, she said. Unless someone had gone through it they could ‘never comprehend’ it, the letter had stressed.
‘We haven’t yet created a safe environment, that’s responsive to the often very vulnerable people who live within it,’ she said. ‘If we focus too narrowly then we’ll miss something that’s hugely important and we won’t reach our aim of reducing the level of deaths in custody.’
More than Treatment
‘It’s much wider than just a treatment need,’ agreed chair of the RCGP’s secure environments group, Caroline Watson. ‘It’s that holistic health, housing and employment need that will stop the cycle of people coming in and out of custody related to their substance misuse.’ Short sentences for drug-related acquisitive crime meant there was very little time for meaningful rehabilitation work, and in the prison where she worked prisoners were released into a number of counties, she said. ‘Multiple locations, multiple services, short times in prison, a transient population and multiple providers.’
Coordinated communication between services was vital, she stressed. ‘We need to build trust and connections not only between people in treatment and providers, but also between the staff of different providers.’ Group work had been badly affected by a prison regime that had locked down for far longer than the wider community, and lack of meaningful activity remained a key driver of prison drug use. Pilots of long-acting buprenorphine – either weekly or monthly injections – were helping to give people an opportunity to connect with community services on release and lessening the risk of dropping out.
When it came to reducing demand, many prisons had enhanced airport-like security and trained drug dogs, partly to address the issue of staff bringing in drugs. ‘But people are ingenious and prisons are being targeted as institutions where serious money can be made,’ said Lyon. ‘The x-ray scanners have proved useful but engaging people in something that provides a bit of hope and sense of future is much more important. I think too often people think that because you’ve got someone detained it’s a brilliant treatment opportunity, and it can be. But the mistake is when the courts see it as a potential treatment centre.’
This was ‘frankly disastrous’, she said, given the pressures on the prison service, very low levels of staffing, overcrowding and extension of remand. ‘It’s the last place one would see as a treatment centre, either for substance misuse or mental health. It’s really important that the courts get a sense that there are real options in the community that work very much better for people who are just getting pulled into the criminal justice system.’
Public Health Approach
Although the Scottish Drugs Deaths Taskforce’s role was to focus on the recommendations it could make within the current law, said Dr Catriona Matheson, its chair and professor of substance use at the University of Stirling, it was clear that ‘we need to move towards a public health approach and away from this crime and punishment angle’. That would ‘allow us to treat people with dignity and respect and help them to thrive. We need to talk about changing the culture around the law and asking the fundamental question – why are we criminalising people with complex needs who experience serious disadvantage?’
No deterrent
The arguments for decriminalisation were based on looking at the failings of criminalisation, senior policy analyst at Transform, Steve Rolles, told the conference. ‘The concept of the deterrent sits at the heart of UK policy, but criminalisation is not an effective deterrent. The evidence is simply not there.’ Criminalisation was, however, actively harmful, with the burden falling most on marginalised and vulnerable communities. It could also increase health harms as people were reluctant to approach treatment or emergency services, and it pushed drug use into higher risk, unhygienic environments.
Policing failure
‘We’ve issued 3m criminal records since the Misuse of Drugs Act was brought into force in 1971,’ said Release executive director, Niamh Eastwood. ‘Criminalisation undermines health, creates further harms and contributes to further inequalities.’ Those targeted by drug law enforcement were mainly young people, people of colour – particularly black people – and those living on the margins, such as people who were street homeless and didn’t have private spaces to use drugs. ‘So while drug use is ubiquitous, drug law enforcement is not. This really matters when it comes to policing,’ with the vast majority of stop and searches carried out on the street related to drugs – primarily possession offences for personal use.
The stigma linked to criminalisation was also hugely powerful. More than half of people who died a drug-related death in England and Wales hadn’t been in contact with treatment services for the last five years, she said. ‘You have to ask why. When you are first and foremost seen as a criminal you are less likely to access the treatment services you may need.’
In the past five years, almost 6,500 people in England and Wales had been sent to prison for possession of a controlled drug, with nearly 80 per cent never convicted of drug possession before. When decriminalisation models were done well, with investment in treatment and harm reduction, then ‘we can see really positive outcomes. An environment where you don’t treat people like criminals means it’s much more likely they’ll access the support they need.’
Drug Diversion
Drug diversion schemes were now in place in some form across around 12 police authorities in the UK, however, said Rolles. ‘It’s in the new drug strategy, it’s one of the Ds in the government’s flagship ADDER scheme, it was recommended in the Carol Black review. The government doesn’t particularly like to talk about it, certainly as a form of decriminalisation, but it does seem to be edging towards becoming national policy, and the better schemes can be seen as a form of de facto decriminalisation. The good ones are largely indistinguishable from the experience you’d have if you were caught in possession in Portugal.’
So what were the obstacles to wider change? ‘Why are we only limping towards decriminalisation when so many other countries support it?’ he said. Simplistic drug war narratives were still persuasive in the public domain and needed to be challenged, and there was also lack of engagement from key professional groups. ‘Doctors, GPs, medical professionals have an authority in the public and political debate. Unlike politicians or journalists, they’re trusted voices, and when they speak out for change people listen.’
They needed to use their voice to advocate for change, he urged, and while some of the royal colleges supported decriminalisation, other organisations had no public position on it. ‘It’s just not good enough. If you don’t have a position on decriminalisation by default you tacitly support criminalisation of a key vulnerable population.’
Change Grow Live explains how three of its services have recently achieved micro-elimination of hepatitis C: West Kent, Reading, and Bromley.
When we say a service has micro eliminated hepatitis C, that means it has reached these targets:
100% of people using the service have been offered a hepatitis C test.
90% of these people have then been tested.
75% of people who were diagnosed with hepatitis C have started treatment.
Hitting these targets is a major achievement for each of these services, and for our role in supporting the NHS in its aim to eliminate hepatitis C as a major health concern.
Find out more about their incredible achievements below.
Reading Drug and Alcohol Service
In March 2022, our service in Reading became the first substance misuse service of its size nationally to achieve micro-elimination.
The service’s success was aided by a lot of hard work from Senior Healthcare Assistant Safina Shahin and the whole team, as well as key partnership working with the local hospital, in particular Dean Linzey, and support from Chrissie Guard of the Hep C Trust. The new approach to hepatitis has already been very well received by the people using the service.
Service Manage Lynn Taylor said: “This is an amazing achievement for the people who use our service in Reading. I am incredibly proud of our whole team and particularly thankful to Dean, Safina and the Gilead team who continued to push Hep C testing and treatment to the top of the agenda for Reading, helping people to become healthier and happier and gain more control over the direction of their lives.”
West Kent Drug and Alcohol Wellbeing Service
Following on from Reading, our service in West Kent also hit the same milestone. This made them the first multi-hub service from all providers in England to reach this major achievement.
Lead Nurse Jo Brown said: “When I heard we’d reached micro-elimination, it almost didn’t sink in. Over two years of hard work had come to fruition!
There are so many elements to this journey, from regular meetings with our colleagues in Gilead, the Hep C Trust and King’s College Hospital, to the support of all our management team, nurses, doctors, administrators, keyworkers, volunteers. Our Senior Data Analyst Sarah Bush also played a huge behind-the-scenes role checking the hepatitis C data month in, month out.
We’re a large service over three sites, so we had to keep momentum going. There is definitely healthy competition between the three hubs, so our Service Manager Clare Begent and I used this to our advantage! We set some in house goals and incentives as well as offering our clients a voucher to be tested.
I remember one of the nursing team saying to me over a year ago ‘I want to be able to say that during my career I played a huge part in the eradication of hepatitis C, how brilliant would that be?’”
Over the last 20 years the UK prison population has almost doubled. With a squeeze in the public purse, one of the casualties has been projects that support people out of prison and back into their communities. The current adult reoffending rate stands at 47 per cent, so what is being done to understand the barriers facing people leaving prison and what help is there to overcome them?
One project in Devon, run by EDP Drug and Alcohol Services (now part of Humankind) is working to provide intensive, tailored support in the weeks that run up to – and on the day of – a prisoner’s release, and it is attracting the attention of funders and commissioners alike.
Transition
The Departure Lounge is based at HMP Exeter, a busy remand prison where an average of 92 prisoners are released each month. EDP Drug and Alcohol Services has worked with a range of community partners for over three years to design and trial innovative, holistic ways to support the transition from prison to community. The result is the highly successful Check Out and Departure Lounge services that are commissioned by the South West Reducing Reoffending Partnership.
There is a lot to plan in supporting someone back into society from the prison environment. They must secure housing and employment, check in with probation, reconnect with families and with communities and life outside, and for some they also have to connect with their local substance misuse service. All of this can be extremely daunting and even overwhelming. Staff use the conversations they have in the Check Out Lounge about the support on offer as a way to identify those with the most complex needs. They can then tailor the support accordingly.
It can be notoriously difficult to get people to open up about their situation and reach out for help, which is why the Departure Lounge team have nurtured mentors to play the role of reducing reoffending champion. They instigate conversations with the men and encourage them to see the benefits of becoming actively involved in their own release. If someone is feeling particularly anxious, they sit with them while they have their conversation with a support organisation to ensure that their voice is heard and understood.
The Departure Lounge’s current reducing reoffending champion (RRC) says ‘from my experience, most people re-offend due to lack of support and accommodation so they get influenced by doing the wrong things to survive. However, most prisoners are keen to become a better person and also be supportive to the community if given the opportunity’.
The RRCs provide support on a number levels – instigating conversations, helping to fill out forms when people can’t read or write, signposting people to the correct support, passing on experience and knowledge or sometimes just providing a prop for people feeling anxious.
The Check Out Lounge is a multi-agency event for prisoners running three or four times a month where prisoners can meet with providers from their local community.
Check Out Lounge
The journey out of prison at HMP Exeter begins a month or so before departure day. Prisoners due for release are invited to the Check Out Lounge, a space for prisoners to meet with many of the agencies that they will need to engage with on their release. These meetings are a combination of in-person, telephone and video conference. Men can call out to these agencies on designated days and speak to specialist staff who will ensure that they are well prepared for the challenges and logistics of integration back into their local community.
Throughout the year there are also a number of hosted conversations with key support organisations. These used to be as part of a community fayre, where men could circulate around the room and ask questions of community organisations including housing, employment, education, substance misuse and debt management. Since COVID these have been done via phone out, from people’s cells and also by video link from the legal video suite area in the prison.
They are also themed to ensure that all aspects of the process of applying for and receiving accommodation, employment and other support issues are covered. These phone out days were advertised through electronic kiosks on the wing landings and by a flyer delivered to each cell.
Housing Matters
Check Out Housing Matters is a more bespoke service. Individual invitations are given to up to 30 prisoners to have a 15-minute video link with their local housing team or probation housing support. They also have follow-on time to meet and discuss issues and concerns with their case manager. These are run twice a month to ensure that all those who are eligible for release in the coming month can get the support they need.
The value of these conversations is the way that they can help people manage their expectations, understand the steps that they will have to make to get what they need and set manageable and realistic goals. It also helps to make men feel a part of the process and that they have a voice. Feedback from the men is also positive. ‘Good news – there is loads of possible help’, ‘I feel this time I was listened to more about my health situation as it wasn’t put on record last time’ and ‘I can see a solution (if approved by probation)’.
Job Fair
With face-to-face Check Out events now able to be hosted again the most popular are Check Out Work Matters and Check Out Job Fair which offer support in finding employment and training and links with potential employers and agents. The feedback is positive with men lining up jobs, arranging follow-on calls, speaking to employment agencies and using an in-cell CV pack (developed by the Departure Lounge team) to tease out skills and experience that help with the application process.
Departure
When the day of release comes, the departing prisoners are invited into the Departure Lounge for on-the-day essentials, like phone charging, clothing and transport. The reality for people stepping outside the prison gates is that all they have with them are the prison clothes on their back and a carrier bag of possessions that were confiscated when they were arrested. That could have been months or years back, so items like mobile phones will have long since lost their charge. It could also be a cold winter’s day – no time to be venturing outside in a thin tracksuit. So the first thing that the Departure Lounge offers is highly practical, or additional items of clothing, water bottles and food for those taking long journeys. The team also look up train times and ensure that the men know where to go for pre-arranged appointments with substance misuse services and probation.
Departure day begins early for the Departure Lounge team. While prison leavers wait in reception to be discharged, staff continue to coordinate support, ensuring medications and prescriptions are in hand and talking to the men about getting home. Where possible Departure Lounge staff carry out an early morning check alongside the custody discharge co-ordinator nurse and reception staff to ensure continuity of care between substance misuse treatment in prison and in the community. This ensures that prisoners do not leave without having received their prescribed dose or onward prescription and a naloxone kit.
After stepping over the threshold, prison leavers are then invited to the visitors’ centre outside the prison gate. Over a cup of coffee Departure Lounge staff offer practical information and advice. Only around 22 per cent of people being discharged from prison who have come through the Departure Lounge have a phone in their possession, so part of the package of support involves donating some phones to those most in need. The final stage of support involves follow-up calls in the weeks after release. Staff invite feedback and offer brief interventions and encouragement.
Confidence, resilience and success
It’s clear that the Check Out and Departure Lounges are increasing people’s confidence, resilience and chances of success when they return to their communities. Addressing two of the most pressing concerns – housing and employment – is having a hugely positive impact in supporting people back into a more settled way of life. The current reducing reoffending champion sees the benefits of his work every day. ‘Through my job role, we have helped many prisoners get accommodation with the help of local councils, and through the hosted series of job fair events we connect prisoners with potential employment and services.’
Pete (not his real name) was a prolific reoffender. He first came into contact with the Departure Lounge when he was handed a flyer about one of its many services, Ask More Phone Out support. One of the numbers on the flyer was for Konnect Communities in Cornwall, an organisation that supports prison leavers back into local communities and into employment. Pete had a really positive conversation with the team at Konnect and it was felt that further contact would cement the next steps for Pete as he prepared to leave prison.
The next available support came via the video link facilities at the prison when Pete was able to benefit from a Check Out Housing Matters session. Following a very successful virtual conversation which further improved Pete’s rapport with Konnect and other services that could help him settle into his local community, Pete was feeling confident about his future opportunities for the first time in a long time.
He then came to the first two Check Out Lounge face-to-face events during October and November where he met properly with Konnect. On the day of his release, Pete visited the Departure Lounge and was met by his family. He was provided with a mobile phone so that he could stay in touch with Konnect and since then he has continued to engage positively with them and is transforming his life. He is supporting himself and others in his family which has meant that he has greatly reduced his risk of reoffending.
Pete is genuinely flourishing and the credit for this is largely down to a new sense of self belief and confidence as well as the contacts he made through the Departure Lounge services which helped him find the right connections back into his local community.
Kerrie Clifford is marketing and communications manager for EDP Drug and Alcohol Service (part of Humankind)
If you’d like more information about the Departure Lounge contact marceva@edp.org.uk
Our challenge in turning experience into expertise
Time and again we hear of people failing to cope with the transition from prison to the community and heading back through the revolving door.
Why? Because they haven’t been equipped, physically or mentally, for their onward journey. The Departure Lounge (p6) is a coordinated approach in action, from making sure prisoners leave with the essentials to connecting them to tailored onward support.
Often problems are so complex that people need immediate intensive support on discharge from prison or hospital, and we can see what a vital difference this makes (p10 and p20).
The other essential element is, of course, meaningful employment (p8) – vital to treatment outcomes and recovery, transformative in building self-worth, and providing socialisation and structure. Visiting the Medway peers this month gave us the opportunity to see this process in action (p12) with a team who have turned lived experience into expertise and ambition.
Of course all of this throws up many issues for our workforce (p14) and prescribing regimes (p22), and it’s important we examine and debate the challenges ahead.
Phoenix’s Making rehab work report looked at the state of residential treatment provision in England. Liam Ward explores the benefits residential can offer to people with experience of the criminal justice system.
The experiences of people involved with substances, crime and the justice system are complicated. Drug offences accounted for 16 per cent of all prison sentences in the UK in 2021, and this figure does not account for the number of violent or acquisitive crimes where substances were involved. There is also growing concern for people exposed to substances during a custodial sentence, with UK government statistics showing that between 2014 and 2019 the proportion of people who developed a drug problem while in custody doubled from 8 per cent to 15 per cent.
At Phoenix Futures our residential treatment services welcome residents directly from prison and many more who have had lived experience of the justice system in their past. To even talk about crime can feed into a stigmatising narrative that some people in society use against our residents, and so some of our current residents were kind enough to share their personal experiences to help us explore these complex issues.
Chelsea
Chelsea began taking drugs at 15, and by age 19 had received her first prison sentence. The following 20 years she described as a ‘revolving door’, only staying out of prison for a few months at a time before returning. She spoke of the complicated relationship she had with prison. ‘Sometimes it was a relief to go back,’ she said. ‘Because I couldn’t get to rehab, I treated prison like a rehab. I knew I could get drugs in there if I wanted to, but I never chased it. I was actually clean when I was in there, I did well. Whenever I came out, my life was chaos.’
I asked whether prison had helped prepare Chelsea for rehab in any way, but she was keen to emphasise the vast difference between the two settings. ‘I thrived on the structure, the routine, the discipline in jail, but in there nothing is expected of you. It’s not like being in rehab, where from the moment you wake up you have to think about how you feel and how you act. In jail you have to put up a front and not let your guard down in order to protect yourself.’
Kelly
Kelly had a similar experience, using heroin at 14 and continuing until the day her son was born. Her first prison sentence came at age 17, and a further thirteen periods of imprisonment followed. ‘In prison I had walls and defences up. I wouldn’t stop and think,’ she said. ‘In there you’re surrounded by people who don’t want to change. I wasn’t happy in that life, but you end up just accepting it.’
Many of the behaviours Kelly had adopted in prison were carried into her life after release, and despite her desire to access rehab with her son, it took some time for her to adjust. ‘When I first came to rehab, I would kick off straight away if I didn’t like the answers from staff, I couldn’t keep my mouth shut,’ she said. ‘But once you’ve built the trust, it is massive. In here you’re encouraged to change and challenge your behaviours, and you don’t realise the change until it’s done. Without my son I’d still be on the same path, using and going in and out of prison, Time is big, you don’t realise it’s running out. If I could do it over again, I would have surrounded myself with people who were better for me.’
Andy
Andy had spent several years in prison prior to coming to rehab. ‘By age 40, I’d spent 20 years of my life in prison,’ he told me. ‘There were times when I got out and I wanted to be back inside. I found the outside world alien and hostile. In prison there was a sense of belonging because people thought like me and had a similar lifestyle.’
Andy explained how his childhood experiences contributed to the intertwining of drugs and prison in his life. ‘I lost my mum to a heroin overdose. The year after that I went into the care system,’ he said. ‘I didn’t use drugs up to being 15, but there was a situation where I smoked heroin with an older friend. Addiction set in straight away, then I got my first prison sentence for stealing.’
Andy’s life from this point onwards was a repetition of the same cycle of drug use, crime and prison time. ‘When I was clean, I felt like I couldn’t cope. I had no skills to be a productive member of society. I had no responsibility. Prison was my parent in a way.’
Andy spoke at length about the circumstances that led to his final prison sentence before coming to rehab. He lost someone close to him, and through an ill-fated error of judgement became involved in a murder enquiry after helping an acquaintance avoid the police. ‘I went to prison, but I was found not guilty during the trial. Whilst awaiting the trial I started working with a drugs worker in prison. For the first time in my life, I became honest. I would always tell lies, cheat, steal, but something changed within me. When I got to rehab, I was determined. I adhered myself to the programme. I put 100 per cent in. I wasn’t going back to that life. I couldn’t say I wanted my life back. I never had a life. I wanted to start again.’
As our conversations drew to a close, I asked what next for the three of them. ‘I just want to be a mum to my little boy. I want to do the school run, take him to his hobbies, enjoy life,’ said Chelsea. ‘I hate the word normal, but I want a bit of normality. I want to be a mummy.’
Liam Ward is residential marketing manager at Phoenix Futures
Kelly too echoed that same word. ‘I want a normal life. Go on holidays, make a business, hold my head up high as I walk down the street. I feel free. ‘
‘I always say I’m one of the lucky ones. I really mean that,’ said Andy. ‘Now I have goals, I have aspirations, a belief system, integrity, morals.
‘I look at my story and what I’ve been through emotionally, mentally and physically and my goals now are to help people who suffer with addiction,’ he said. ‘I want to have a beautiful family, earn my own money. I want to use my experience, my story to help people.’
There has been a staggering increase in deaths among people who are homeless. Photo by PIXNIO
The number of deaths among people experiencing homelessness rose to almost 1,300 last year, according to new research from the Museum of Homelessness charity. The museum’s ‘Dying Homeless’ project recorded 1,286 deaths across the UK, more than 30 per cent up on 2020 and a ‘staggering’ 80 per cent increase on 2019.
While just seven deaths were the result of COVID, cuts to substance misuse and mental health services had ‘taken their toll’, says the charity, with the result that that ‘too many people don’t get the support they need’. Of the cases where the charity had confirmed the cause of death, more than 40 per cent were related to drug and alcohol use and 12 per cent to suicide. Most of the drug-related deaths took place in temporary, hostel or supported accommodation, rather than on the streets, with particularly high numbers in South Lanarkshire, Exeter, Southampton, Stirling, Hull and Leeds. Cuts to housing services have also had a significant impact, with many of the deaths taking place in ‘unsafe, unregulated, taxpayer-funded accommodation’.
Jess Turtle: calling for a confidential inquiry into the deaths
The figures – which represent a death occurring every seven hours on average – are based on more than 300 Freedom of Information requests as well as coroner reports and other sources, and include people sleeping rough as well as those in emergency accommodation or other insecure settings. The actual number of deaths is likely to be far higher, says the organisation, as many local authorities – including the UK’s second largest city, Birmingham – did not respond to FOI requests.
‘These findings are a hammer blow,’ said the charity’s co-founder, Jess Turtle. ‘Government neglect means things keep getting worse with new provision for mental health, addiction and social housing failing to make up for previous cuts. Ultimately, the government can’t fix what it doesn’t understand. There needs to be a confidential enquiry into the deaths of homeless people to allow an honest appraisal of what’s happening to the UK’s most vulnerable people. There should also be mandatory fatality reviews for all local authorities – so lessons can be learned from each death.’
Two of SIG’s Penrose groups in Luton are using a group art project to promote mental health.
Since the war broke out in Ukraine, many organisations have mobilised and started fundraising and donation efforts to assist those displaced or otherwise affected by the war. But two of our Penrose groups in Luton have focussed their efforts on mental health.
The Penrose Pom Poms for Peace campaign began as part of the art activity which is run at the Friday Connects Group.
When the war in Ukraine began, the group along with Penrose Roots club members started to think about peace in this terrible time, and about those fleeing Ukraine as well as those affected by war across this world. They decided that they would start to make Pom Poms for Peace.
The group used mainly donated wool, added tags and their logo and started to give the pom poms out to family and friends as well as to leave them in random places in Luton for people to collect and take home.
The question could be asked, how does what started as a simple group art project really help with the current situation?
Firstly, the group hopes that it may bring some joy and colour to those who received or found them. Secondly, they hope that it may encourage people to realise the importance of peace whether this means in time of war or personal peace of mind. They also hope that it may make people think about donating to a one of the many causes, whether financially or by supporting with donations of clothing and supplies to local Polish centres which are making regular trips to the Polish border.
But it is also important that as a community group they worked together, enjoyed making the pom poms, had much conversation and now have the satisfaction of giving them away or randomly leaving them around the town, which means they get to exercise too!
Elizabeth Aldous, volunteer and community programme coordinator said: “I have personally made more than 200 pom poms which has kept me very busy AND are taking over the house! We may also have some at our Spring Fair which is approaching. As somebody who has volunteered with refugees fleeing the war in Syria and Afghanistan, I wish to go and help with this crisis in Poland or Moldova. But in the meantime, I shall continue to make Pom Poms for Peace.”
These pom poms may not make a huge difference but even though they just make someone smile, that would be enough.
With You’s Robin Pollard asks, how do we improve access for women experiencing domestic abuse?
“Many women have a deep distrust of services, often due to bad experiences with social services. It can mean it takes a long time to develop trust.”
For people who need support, coming to our services can be life changing. However, for some people our services are still too hard to access and this is especially true for women who have experienced domestic abuse.
At the heart of the experience of domestic abuse is fear, and this is something often experienced on a daily basis. Whether it’s fear of a partner, fear of losing a home, or fear of being stigmatised by family and friends. This is exacerbated by the reality that women with experience of domestic abuse are far more likely to be drug or alcohol dependent but are more likely to experience poorer treatment outcomes.
At With You, we’re always looking to better improve the holistic support we provide people and taking the fear out of the process of stepping forward and seeking support is a crucial step.
Though there are things we do very well, we also know there are things we can do better.
Integrating services
For women who may have had negative experiences with services before, drug and alcohol services offer an essential and critical referral route to domestic abuse services. That’s why where there is a clear need, we try to bring domestic abuse support and drug and alcohol support under one roof.
We know the value integrating these services can bring. Our new service in Redcar & Cleveland is expanding to include domestic abuse support. This new integrated model works in partnership to offer refuge to women and children fleeing domestic abuse, as well as advice and support. It will drastically improve access and engagement for women whose experience of domestic abuse and related trauma has made getting support and treatment even more challenging.
Embedding knowledge and training
Being a front-line recovery worker isn’t easy. It requires a unique skill-set which is often misunderstood and under-appreciated. In order to identify and support women with experience of domestic abuse, frontline workers need to know how to ask the right questions, in the right tone, and know what to do with the information disclosed to them.
Our recent research heard from professionals that the more they understand about a woman’s experience of trauma, the better and more appropriate the support they can provide. This results in more trusting relationships, stronger personal connections, and better opportunities to help women holistically address their problems.
To ensure we are delivering a trauma-informed service, frontline workers need to be trained not just to recognise trauma, but to understand it too. Training should address: recognising and understanding domestic abuse, sexual exploitation and adverse childhood experiences and safety planning for women experience domestic abuse.
Mohammed Fessal looks at the evolving role of buprenorphine in medication-assisted treatment in the UK and how it has benefitted Change Grow Live’s service users
Mohammed Fessal is chief pharmacist at Change Grow Live
People seeking medication-assisted treatment (MAT) for management of opioid dependence have two primary options – methadone and buprenorphine. Maintenance treatment with methadone was commonplace in the late 1980s into the 1990s, with buprenorphine introduced as an additional option under the brand name Subutex in 1998 and later becoming available as a generic preparation. Since 2006, a combination product called Suboxone containing naloxone in addition to buprenorphine has also been available, which has a place in treatment where there is a risk that buprenorphine alone may be misused through intravenous or intranasal use.
Both methadone and buprenorphine are effective in achieving positive outcomes in opioid-dependent individuals and are recommended in national guidelines, including the Drug misuse and dependenceguidelines and NICE. Decisions relating to medication choice are made on a case-by-case basis, taking into account the person’s dependence history, their commitment to a long-term treatment plan, their personal medication preference and an evaluation of the risks and benefits of each drug.
There is evidence that buprenorphine is associated with reduced risk of fatal overdose during treatment initiation – however there is also evidence that methadone is more effective at retaining people in treatment, and therefore may reduce risk in the long-term. Buprenorphine may be a preferable treatment option for those with children in the home as it presents less risk than methadone due to the different routes of administration. All but three of the 110 UK deaths in under-18s from ingestion of medications used in MAT between 2003 and 2013 were related to methadone.
Buprenorphine has historically been available for use in substance misuse treatment solely as a sublingual tablet, and long-term experience with its use, cost-effectiveness, better safety profile and ready availability has made it the ideal choice to support thousands of individuals.
Espranor
In 2015, a new oral lyophilisate formulation of buprenorphine, Espranor, was launched. A formulation that dissolves on the tongue in 15 seconds, its intended benefits include service user convenience and reduced risk of diversion. In 2017, Change Grow Live conducted a pilot study in four services across the country with Espranor to evaluate its place in treatment, which demonstrated the following outcomes:
Espranor was preferable for service users compared to sublingual buprenorphine as it dissolves more quickly on top of the tongue. This results in a faster administration time and reduced waiting time in the pharmacy for those receiving supervised consumption.
Pharmacy teams also preferred it to sublingual buprenorphine as it reduced the time they spent observing MAT doses, particularly in pharmacies where they observe a lot of people receiving MAT each day.
Anecdotal evidence that Espranor was associated with reduced risk of misuse and diversion.
In the UK, supply issues saw the market price of generic buprenorphine increase unexpectedly by more than 700 per cent in early 2018, putting unanticipated strain on prescribing budgets. The positive information gathered from the Espranor pilot combined with the impact of this price increase on already limited prescribing budgets – as well as unpredictability in supply of medicines not manufactured in the UK as a result of Brexit – meant that a decision was made to move people taking buprenorphine onto Espranor where appropriate to ensure continuity of treatment. The positive feedback about Espranor from service users, staff and other stakeholders provided assurance that this would be a positive adjustment for service users, and Espranor became the first-line buprenorphine treatment on the Change Grow Live formulary.
Changing people from sublingual buprenorphine to Espranor
In August 2018, just 2 per cent of clients were taking Espranor (a continuation of treatment from the pilot study) with all other people taking buprenorphine being prescribed the sublingual formulation (Figure 1). Those taking buprenorphine who were identified as suitable for moving over to Espranor were contacted individually and the change discussed with them. By April 2021, 78 per cent of people who were taking a buprenorphine formulation were prescribed Espranor (Figure 1). Of note is that 1,932 people remained on prescribed generic buprenorphine – Espranor is not for everyone because of licensed dose limitations, clinical parameters, side effects, religious beliefs or dietary reasons.
A significant benefit of this national switch to Espranor prescribing was that it provided the opportunity to optimise MAT doses in line with the ‘Orange Book’ to a minimum of 12mg buprenorphine daily. Optimising the dose is a huge challenge for individuals who have in many cases been on the same dose for a long period – however with this medication switch the average dose increased from 9.7mg to 10mg between August 2018 and April 2021, and 44 per cent (3,886) of people taking a buprenorphine preparation are now on a dose of 12mg and above, compared with 41 per cent in August 2018.
Bioavailability differences between generic buprenorphine and Espranor mean that the two medications are not directly interchangeable. However some studies suggest that Espranor is no more likely than equivalent doses of buprenorphine to cause respiratory depression – this is due to Espranor resulting in a higher buprenorphine to norbuprenorphine ratio, which is associated with a reduced risk of respiratory depression. With a safety first and learning- based approach, each person was reviewed individually, and their medication and dose adjusted as appropriate, with careful monitoring during the transition period.
More than half of the people who changed from buprenorphine to Espranor remained on the same dose at the point of switching (Figure 2), and a large proportion of people remained on the dose they started Espranor on after 28 days of treatment (Figure 3). A larger proportion of people required a dose change within 28 days of starting Espranor treatment if they changed dose at the point of switching from sublingual buprenorphine, and if people needed to change dose after starting Espranor they were more likely to need a dose increase than decrease.
The feedback received about Espranor from both service users and the people involved in delivering their treatment has generally been positive.
‘It’s easier to take and tastes better [than sublingual buprenorphine].’
‘I really feel good being on Espranor. I feel this has really helped in me being able to fully stop illicit drug use.’
‘I wish I’d been given this years ago.’
For example, one individual has been able to reduce their medication dose from 16mg to 6mg since starting treatment with Espranor. This positive outcome has also been experienced by another person who requested to change from methadone to Espranor, and is since fully engaged in group sessions and proud that they are able to no longer use heroin which they have put down to the change in medication.
An outreach worker reports that people find Espranor less intrusive when doses are being supervised, and that Espranor feels more dignified as people do not have to stand in the pharmacy for a long time waiting for the dose to dissolve. They also echo service user feedback that Espranor tastes better. Staff report reduced diversion risk as a key benefit, and they are more assured that people are taking their prescribed dose.
Buvidal
Drug development in recent years also led to the introduction of Buvidal in 2018, which is a prolonged-release buprenorphine injection administered either weekly or monthly. Buvidal may offer benefits such as reduced diversion or misuse risk, and prolonged partial agonist effect in the event of abrupt treatment cessation – for example, unexpected prison release or hospital discharge – which may lessen overdose risk. Other benefits may include convenience for the service user, and assurance of adherence to treatment for the prescriber. The safety of Buvidal is similar to oral buprenorphine with the exception of injection site reactions, although long-term safety data is limited to a 48-week long study.
Change Grow Live has conducted a pilot study in two locations to evaluate Buvidal’s place in treatment and has introduced Buvidal across the country to further evaluate the benefits this treatment option has for supporting service users, many of whom may previously have struggled to engage and remain in treatment. The benefits and outcomes need to be weighed against the cost of this treatment, which is much higher than for the more ‘traditional’ MAT options.
Treatment with buprenorphine in specific populations
Prisons
Historically, buprenorphine has not been routinely offered as an MAT option in prisons due to risk of diversion and misuse, and the length of time it takes to supervise sublingual buprenorphine until it has fully dissolved. Espranor may be an appropriate alternative due to its quicker dissolution time, and Buvidal may also have a place in custodial settings where there can be challenges around supervising medicines safely. Prisons in Scotland have offered Buvidal as an alternative to daily supervised MAT, and have found positive effects on wellbeing, reduced illicit drug use, and freeing up of healthcare resources.
Pregnancy
Buprenorphine is not licensed for use during pregnancy, and transfer onto buprenorphine during pregnancy is not recommended due to risk of precipitated withdrawal or inducing withdrawal in the foetus. However, if a woman is stabilised on buprenorphine and becomes pregnant, then therapy should be continued. Buprenorphine does not have adverse effects on pregnancy or neonatal outcomes, and there is some evidence that buprenorphine results in less severe neonatal abstinence syndrome (NAS) than methadone.
Prescription and OTC dependence
People seeking treatment for prescription or over-the-counter (OTC) opioid dependence may respond differently to treatment with buprenorphine (or methadone) than those dependent on heroin, and the evidence base to determine practice is weak. However, it is appropriate to suggest a period of substitution treatment with either buprenorphine or methadone, recognising the benefits and limitations of each.
The evolving role of buprenorphine means people now have a wider range of formulations available to them, making it a suitable medication choice for many people who present for treatment and who previously may not have been an appropriate candidate for buprenorphine. This allows more people to be supported in a way that is optimal for them, and ultimately contributes to their successful treatment and recovery.
This online article is intended for medical professionals and does not recommend one medication over another. If you are a member of the public, always speak to your GP or medical advisor who will recommend the best treatment options available to you.
Phoenix Futures is sharing stories of lived experience of some of the people who have accessed its residential services. This is Kamil’s story.
Every person that we support has their own unique experiences, stories and insights that shared help to inspire, educate and enable better support for others in need of help. Following on from the launch of our Making Rehab Work report, we are sharing the lived experience of some of the people that have accessed our residential services to reinforce the need for equality of access to residential treatment across the country. We thank Kamil for sharing his story and for his honesty and openness about his experiences.
Kamil’s Story
I was born in the Czech Republic, my parents are both from Slovakia but moved there before I was born. Growing up was hard, we were poor, and I experienced a lot of racism. When I was 13, we moved to Derby in the UK. The first few years were nice, I was going to school to learn English and was happy.
By the time I was 16, I had started hanging around with some older boys, smoking weed. I had left school and went to work in a shampoo factory which meant that I had more money to spend on going out and smoking weed. When I was about 18, I went back to the Czech Republic for two months to see a girl, she introduced me to heroin for the first time.
When I came home, I met a new crowd of people who were injecting heroin and I started to do the same. I thought I could handle it, I thought I was invincible. I went on holiday to Slovakia with my dad, so I stopped using, I started to get sick, now I realise that I was withdrawing from heroin but I didn’t understand at the time that I had become dependent.
I carried on using for years. I stole and shoplifted to buy drugs. I met a girl, we had two kids. My daughter was three when my son was born, we had been living with my parents but moved out into our own flat to get some more space. My son became unwell and ended up in hospital for a few months.
My girlfriend wasn’t happy about me using drugs, she kept threatening to leave me. I stopped using heroin when I got a prescription for Subutex, but it wasn’t long until I started using other drugs instead.
Things got worse when I started using Mcat, I was hearing voices and getting paranoid. I thought there were other men in the house and my girlfriend was cheating on me. It wasn’t long before she packed up one night with the kids and left. I was devastated, feeling like I didn’t have anything left to live for so I used more and more. I became homeless and was sleeping rough. Living on the street was hard, but I didn’t know how I was going to make things better.
In 2017 I got a place in a hostel, I made friends with a guy who was a cleaner. I used to help him clean and we would talk, he told me that I needed to go to rehab and do a proper detox where I stopped taking everything, even the Subutex. By that time, I was desperate, so I was willing to give anything a go.
Doing the detox was tough and painful. I went straight from there to rehab in The Wirral. as soon as I arrived, I wanted to leave, I didn’t like it and I didn’t want to stay. I spent months telling everyone I was going home, and I probably would have done, but because I had a problem with my benefits, I didn’t have the money to leave, so I stayed. I got support for my mental health whilst I was in treatment, I was diagnosed with paranoid schizophrenia and have been taking medication since which has helped.
As my graduation got closer, I realised that I didn’t want to leave at all and was desperate to stay. I stayed for seven months in total. When I left the residential, I went into Phoenix supported housing, which was two and a half years ago, and I am still living in Phoenix housing now. Since I left treatment, I have been back to college, passed my driving test and have rebuilt relationships with my family. I volunteer at the residential, supporting people that are just starting their recovery journeys. I want to be an inspiration to them and show them that recovery is possible. I have an amazing life; I know that I will never go back to using drugs again and I am really looking forward to the future.
Recent statistics show that from October 2020 to November 2021, Turning Point’s City & Hackney teams helped over 3,000 residents on their drug and/or alcohol recovery journey.
In addition, front line staff have:
dealt with over 41,000 emails and phone calls
issued over 20,200 ‘scripts
conducted 271 recorded blood tests
received only 16 complaints and
trained over 200 professionals in alcohol awareness and substance misuse.
Deputy Operations Manager, Paul Grannum said:
“We’re really proud of the impact we are beginning to have on the communities we serve. The pandemic impacted services across the board – and we’ve done our utmost to make sure that clients were getting the support they needed.”
London’s mayor should work with the Metropolitan Police to ensure that its officers routinely carry naloxone spray, according to a new harm reduction report from the London Assembly Health Committee.
The committee also want to see consumption rooms piloted in London
Police Scotland recently announced that it was rolling out its pilot naloxone programme across the whole of the country (DDN, March, page 4), following successful pilot schemes.
Naloxone is ‘not as readily available as it should be’ in the capital, says Reducing drug deaths in London, which also calls on the government to introduce a nationwide naloxone programme in England to end the ‘postcode lottery of provision’. The committee also want to see consumption rooms piloted in London, and for drug-checking services to be provided at clubs, music events and other venues.
Just under 10 per cent of Londoners report previous-year drug use, the document states. ‘As a diverse city, with pockets of both extreme wealth and extreme poverty, London has highly contrasting drug use scenes, which differ by local area and by socioeconomic, cultural and ethnic groupings,’ it says. Earlier this year, the mayor’s office was forced to defend its as-yet unapproved diversion scheme in three boroughs for young people caught with cannabis, after media reports that it was planning to ‘decriminalise drugs in London’.
Committee chair, Caroline Russell
‘Too many people are still dying from drug-related causes in London,’ saidchair of the committee, Caroline Russell.‘We investigated how to address this tragedy and find out what practical, life-saving interventions could be used to reduce drug harm in our city.
Our investigation found that naloxone could save someone’s life if it’s used quickly after an opioid overdose. That is why we are urging the mayor to ensure the Met routinely carry naloxone, a simple and proven way to reduce opioid deaths.Additional measures recommended in our report, such as a pilot for safe drug consumption rooms and the introduction of drug checking services, can start to bring down the growing numbers of people sadly losing their lives due to problematic drug use.’
There was an 8 per cent fall in suspected drug deaths in Scotland in 2021, according to the latest quarterly figures. Provisional statistics from Police Scotland show that there were 1,295 deaths last year, compared to 1,411 in 2020.
Two thirds of deaths were among people aged between 35 and 54
The quarterly figures represent deaths that the police suspect to have involved illicit drugs, and are different from the official National Records of Scotland (NRS) statistics which are based on information from death certificates and forensic pathologists. Since late 2018 the Police Scotland figures have ranged between 3 and 6 per cent above the NRS figures, with the NRS total for 2020 recording 1,339 deaths.
As in previous years, men accounted for almost three quarters of the deaths, while almost two thirds were among people aged between 35 and 54. The number of deaths in under 25s fell by 20 compared to the previous year, while deaths in the last calendar quarter were 76 down on the same period in 2020.
New figures from the Office for National Statistics (ONS) on avoidable deaths, meanwhile, show that the age-standardised mortality rates for alcohol- and drug-related deaths in Scotland was 52.1 per 100,000 people in 2020, more than double the 24 per 100,100 rate in England. ‘Since 2012, avoidable rates from these causes increased by 63.3 per cent in Scotland,’ says ONS.
Angela Constance: Death toll ‘still far too high’
Despite the decline the death toll was ‘still far too high’, said drugs policy minister Angela Constance, with ‘much hard work to be done to turn this public health emergency around. Getting people into the treatment which works for them is key and we continue to embed the new medication-assisted treatment (MAT) standards which reinforce a rights-based approach for people who use drugs and the treatment they should expect regardless of their circumstances. We also aim to increase the number of publicly funded residential rehabilitation placements by more than 300 per cent over the lifetime of this Parliament and I will also shortly be announcing a target to increase the number of people in treatment.’
There had been a slight increase in the number of deaths among women, she added, with the government committed to tackling the barriers that prevented them from accessing treatment. ‘One of our priorities is to develop and increase women-specific services, and services to keep children and families together. I am determined that the £250m we are investing in tackling this public health emergency will make a difference and we will continue to prioritise our efforts to turn this crisis around.’
A recent report from Audit Scotland, however, concluded that delivery of Scotland’s drug and alcohol services remains complex, with unclear accountability and difficulties in assessing the effectiveness of the money being spent, despite the government’s pledge to invest £250m over five years. (www.drinkanddrugsnews.com/clear-plan-needed-to-improve-complex-scottish-services). Drug and alcohol data was ‘not good enough’, said auditor general Stephen Boyle, with a lack of transparency and the need for a ‘clear plan’ to improve service provision.
Suspected drug deaths in Scotland: October to December 2021 at www.gov.scot – read it here
Avoidable mortality in Great Britain: 2020 at www.ons.gov.uk – read it here
In this article, Sarah Marsay from Samaritans and Robin Pollard from With You talk about recent work from the Suicide Prevention Consortium to capture the views of people with lived experience of alcohol use, suicidality and/or self-harm.
There is a close, well-evidenced relationship between alcohol, suicide and self-harm. This relationship varies depending on a range of factors, including how different groups of people use alcohol. For example, heavy episodic or binge drinking is associated with increased likelihood of attempting suicide amongst adolescents, while people who are dependent on alcohol are approximately 2.5 times more likely to die by suicide than the general population. In England, nearly half of all patients under the care of mental health services who die by suicide have a history of alcohol use.
Despite these links being well researched and documented, the Suicide Prevention Consortium found the voices and perspectives of people with lived experiences were often hard to find. In 2021, the consortium launched a new project exploring the relationship between alcohol, suicide and self-harm, focusing on the perspectives of people with lived experience and putting their insights at the forefront of our work.
The complex relationship between alcohol use and mental health
From the 125 people with lived experience that completed our surveys, we heard how people had a diverse range of relationships with alcohol, and there were many different ways they viewed the link between their suicidality, self-harm or mental health.
For some people, alcohol helped them reduce their inhibitions, while for others it was a coping mechanism — usually a way of dealing with trauma. Many people were aware of why they drank, and the effect it had on them. This included both the negative impact on their mental health or mood at the time of drinking, but also the longer-term impact, often experienced days or weeks later.
“Alcohol used to take all of the bad feelings away for the moment but always left [me] sad after. Depression hits the day after I drink.”
One of the most common themes we heard was how people used alcohol to cope with other underlying issues. We also heard how support services were sometimes unprepared, unable to understand or unwilling to respond to the underlying trauma.
Alcohol as a barrier to mental health services
We heard how despite alcohol being closely linked to people’s mental health and suicidality, services they accessed struggled to treat them as such. Experiences of support services working in isolation were common. Some people said they felt afraid to disclose their alcohol use when seeking mental health support fearing they could be deemed ineligible for mental health treatment, and/or because they didn’t feel ‘safe’ to do so. Far too many people told us they couldn’t access appropriate support due to strict eligibility criteria, often at a local level, excluding people from the help they need. Their co-occurring needs around alcohol and mental health weren’t treated as a shared responsibility for different services.
However, despite these systemic problems, we did hear examples of good individual practice. Many people in our survey experienced what they felt was good care, and pointed to the expertise, empathy and compassion of individual practitioners who sought to understand their personal experiences with alcohol.
The role of alcohol in suicide is not taken seriously
One of our most concerning findings was that some people who were intoxicated at the time of a suicide attempt experienced dismissive attitudes from frontline professionals who down-played or misunderstood the seriousness of the attempt/intent and failed to offer appropriate support. The persistence of shame and stigma associated with alcohol issues was commonplace.
The prevalence of chronic hepatitis C in England was just over 80,000 in 2020, according to the UK Health Security Agency (UKHSA), down from almost 130,000 in 2015 – a fall of nearly 40 per cent.
The figures show that there has been ‘considerable progress’ towards the target of eliminating hep C as a public health problem by 2030, the agency states.
Deaths from hep-C related advanced liver disease also fell from 482 to 314 over the same period, which exceeded the World Health Organization target of a 10 per cent drop by 2020. ‘Provisional data’ also suggests that there has been a 40 per cent reduction in the number of people injecting drugs, UKHSA says.
The reduction in prevalence is largely a result of improved access to treatment, with almost 60,000 treatments taking place between April 2015 and March 2021. Of the 81,000 people in England estimated to be living with hep C, around 27 per cent are thought to be people who have recently injected drugs, while more than 60 per cent are people with a past history of injecting. Just over 10 per cent are people with no history of injecting drug use.
UKHSA CEO Dr Jenny Harries
More than half of people who inject drugs may have a chronic hep C infection and remain unaware of it, UKHSA estimates, and despite the ‘huge progress’ challenges remain. ‘While effective treatments are available, we need to stop people becoming infected in the first place if we are to eliminate hepatitis C,’ the agency states.
‘It is really encouraging to see cases of chronic hepatitis C declining in England,’ said UKHSA CEO Dr Jenny Harries. ‘We must keep pushing this trend downwards – too many people continue to be affected by this debilitating but preventable condition. Hepatitis C treatment has improved dramatically over recent years. Latest treatments are effective and well tolerated, so if you have been at risk or tested positive in the past don’t delay visiting your GP.’
Join the fight for elimination! See the latest supporting hepatitis c testing and treatment
‘In England, we are on our way to eliminating hepatitis C as the number of deaths continue to decline and direct acting antiviral drugs are available that will clear the virus in around 95 per cent of people who complete treatment,’ said UKHSA clinical scientist Dr Helen Harris. ‘But many people remain undiagnosed, often because they have no symptoms or are unaware that they have ever been at risk. If you have ever injected drugs – even if it happened only once or years ago – you could be at risk of hepatitis C. If you think you could be at risk, speak to your GP and get a free test.’
‘From the moment I arrived I was surrounded by energy’
We wondered if it would ever happen – and then there we were, with everyone pouring through the doors of our first conference for three years. Overwhelming and exhilarating. In this issue
you’ll find all kinds of impressions of the day, but for me the highlights, alongside inspiring speakers and our team of amazing volunteers, were the connections – reunions, introductions, endless possibilities for working together and sharing ideas.
More pictures, presentations, and conference footage coming shortly.
How amazing to see everyone in real life!
Loved seeing everyone and we really appreciate everyone’s efforts to get there during the rail strike.
Thank you SO much to our amazing speakers, exhibitors sponsors and to all of you who came and made the day special. Massive thanks to our volunteers who helped beyond measure.
Please post your photos on our Facebook page – we’d love to see them!
Lots more pics coming soon, plus video, speaker presentations and write-up of the day.
If you’d like to contribute your experiences of the conference to our special issue, please email them by 1 July! Send to claire@cjwellings.com
If you have booked a place, exhibition stand or group of delegates venue details, information for exhibition stands and the form for adding delegate names is here.
DDN Conference 2022 – travel update
We’re really excited about this year’s conference – the biggest best one ever! We want to put everyone’s mind at rest that the prospect of train strikes, just announced, will not affect it going ahead. The venue is on main road networks and has a large free car park and the vast majority of delegates and exhibitors drive to the event. If you were planning to travel by train we hope you have enough time to make alternative arrangements by coach or car. If you are driving and have space, please use #ddnconf to offer a lift – and if you need one, please use the same hashtag to ask! All together now… LET’S DO THIS!
Venue details, timings, and information for exhibitors is here
The Drink and Drugs News National Conference will be held on 23 June 2022 in Birmingham.
The event will bring people with lived experience, patient groups, treatment providers, members of the recovery community and policy makers together to strive to provide better, fairer treatment for all.
The conference regularly attracts in excess of 500 delegates from across the UK. Like the magazine, the conference creates an open forum for debate.
The large exhibition area gives scope for a vibrant networking forum that comprises a wide variety of stalls and information booths, surveys and academic research opportunities, meetings, therapies, sports taster events and a film festival.
This is the must attend event of the year for services, local groups and individuals.
Individual delegate places are £75 for volunteers and people with lived experience or £135 for professionals. Price includes refreshments and the famous DDN Birmingham curry!
Individual tickets can be booked via credit card here.
If you would rather be invoiced please email ian@cjwellings.com Please title your email DDN Conference Tickets 2022 and please put your contact details, the amount of tickets required and the invoicing details in the body of the email (you don’t need to supply delegate names yet if you don’t have them). You will receive confirmation and an invoice within a couple of days.
The DDN event is best experienced as part of a group and we can offer reduced rates for group bookings from local peer-led organisations. Please contact ian@cjwellings.com 07711 950 300 for details.
If you have booked a place, exhibition stand or group of delegates venue details, information for exhibition stands and the form for adding delegate names is here.
Please use the button below to book individual tickets for the event. For group booking please contact ian@cjwellings.com 07711 950 300
Be part of the vibrant exhibition area, showcase the services you provide, network with treatment providers, policy makers and people who use services and support this unique event.
Where? New Bingley Hall, Birmingham, B18 5PP. There is ample free parking and the venue is a short cab or bus ride away from Birmingham train stations.
When? 23 June, 2022 10am – 4pm (registration from 9am)
Who should come? People with lived experience, recovery groups, treatment providers, policymakers, commissioners, activists, suppliers. Everyone who is passionate about providing better, fairer treatment for all.
What’s on? This is a chance to meet services, and community groups and share innovation and best practice. There will be a full programme of presentations, interactive sessions and learning activities as well as a large exhibition and networking area. Full programme here.
How much? DDN is a free magazine and self-funds both the publication and the event. We make the ticket price as affordable as possible, and also offer free stands for groups attending. Individual delegate ticketsare priced at £75 – £135 and are on sale here. Please contact ian@cjwellings.comto find out more about exhibitor and group bookings.
Funding Most delegates are funded by their local service or attend as part of a group. In the first instance please contact your service provider to see if they will fund your place or if you can be part of their group. Dependent on sponsorship DDN might have some bursary places available, please get in touch if you are struggling to pay to attend.
Exhibitor information The event is the perfect place to showcase your product, services, or demonstrate what is happening in your area. Please get in touch to find out more.
In honour of International Women’s Day, Social Interest Group is this week running a series on the women of SIG.
In the third of our series of profiles for International Women’s Day week, today we profile Veronica Claridi.
Imagine growing up multiracial, multilingual, between countries, between cultures, and never quite feeling like you fit in. Then imagine using those conflicting parts of you to change the narrative of your life and then using them to become that woman who can put herself in another’s place and help those moving to a new country to settle well. All whilst building a career in which you help others to reclaim their lives. This is Veronica’s story.
About Veronica
Veronica is the field care supervisor for Penrose Care and Support Service (PCCS). She grew up between Brazil and Italy with her Italo Brazilian father, Jewish Italian mother and older sister. Her parents were, and still are her role models, have been married for over 40 years and still love each other like the first day they met. Her father has always been very passionate and open to learn and discover new things and her mother a strong, independent and direct woman. Their influence can be seen in the way Veronica lives and her love of life. Her family and friends describe her as kind, passionate, loud, honest and opinionated – with a hidden talent for carpentry.
Veronica and her ex-partner suffered through years of struggle with multiple miscarriages and failed IVF cycles. Finally, five and two years ago they became mummies to two wonderful boys who they are extremely devoted to. At times, especially since her partner moved out of London, it gets demanding and stressful trying to balance work, motherhood and living a normal life. But she wouldn’t change things and sees her children as the best part of them. In fact, her children have been the biggest influences in her life. They taught her patience and without mercy, pushed her to be a better person. She used to live for the day and partially because she moved around a lot and lived in many different countries, before settling in London, never felt at home. Her children though, now make her feel at home, wherever they are, as long as they are together.
Veronica grew up between the South of Italy, North of Italy and Brazil. Most cities in Brazil have a high index of criminality and social inequality, so growing up, although very privileged compared to others, Veronica witnessed a lot of social injustice. The family then moved to Italy, thinking that it would be different, and started again in Naples. It was not much different. She spent five years secluded within the walls of their apartment, with an invisible curfew, that would start when they returned from school to the next morning. The streets were very dangerous, with shootings and kidnappings being commonplace.
The family then moved to Milan, where they were constantly marginalised because of her father’s skin color or the fact that their Italian, at the beginning was not perfect. She felt like she had no clear identity or culture. They spoke three different languages at home and practiced two different religions. This meant celebrations and observances that her friends never heard about but which her and her sister had to participate in, regardless. This led to Veronica mixing with others that, like her, felt lost. She eventually channelled her experiences into wanting to help others.
Veronica spent many days between Italian public libraries and parks and got involved in the student’s political movements and became an integral part of what used to be a way of living. They believed and supported social equality, the right to live a good life and the right to be cared for, socially and medically. They thought they were going to change the world, while sipping Earl Gray and smoking cigars. It was very much in fashion at the time, and definitely a political stand! This led Veronica to study sociology at university and to later move to London, which is more multi-cultural.
A new direction
Veronica worked in different settings and different industries, but care has always somehow been part of her life, whether it was a paid job or volunteering. She loves her job with SIG! She said: “I love everything that it stands for. At times I wish that days were longer, and I could be more in the community. While working, I get to really know other people’s struggles, success and progress and, knowing that I am part of it, gives me an immense sense of joy. I try not to get too emotionally attached, but I feel sometimes, it is inevitable.”
Veronica is also proud of the charity work she does hands on for refugees. She built a Hub in her area with few others, where they collect clothes, medicines, toys, blankets, etc. They take the donations to borders such as Dover and Calais in France and support families who have crossed the borders and are now living in London.
Although the last two years have been challenging for everyone, in mental health, the struggle to continue to provide high quality care, has been particularly difficult.
Find out more about Veronica and read more inspirational stories from The Social Interest Group’s women here.
DDN magazine is a free publication self-funded through advertising.
We are proud to work in partnership with many of the leading charities and treatment providers in the sector.
Bonne Terre Limited, which trades as Sky Betting and Gaming, has been fined just under £1.2m for sending promotional emails to customers who had self-excluded or opted out of receiving marketing, the Gambling Commission says.
A promotional offer reached many people who had unsubscribed from marketing.
The company distributed a Sky Vegas promotional offer of ‘Bet £5 get 100 spins’ to more than 41,000 customers who had self-excluded and almost 250,000 who had unsubscribed from marketing emails, the regulator states. Self-exclusion is used by people who feel they are struggling to control their gambling to request that the operator refuse their custom, a facility the Gambling Commission requires all operators to offer. Contacting these customers constituted a breach of licensing conditions aimed at ‘ensuring gambling in Britain is socially responsible’, the commission said.
Earlier this month 888 UK Limited was fined almost £9.5m for ‘social responsibility and money laundering failings’ including not effectively identifying players at risk of harm, giving a customer known to be earning £1,400 a month a £1,300 monthly deposit cap, and not carrying out a customer interaction with someone who lost almost £40,000 in six weeks during the pandemic.
Read our feature in the latest issue of DDN.
In the March issue of DDN, campaigner Kelly Field describes how she spent more than £10,000 on a single credit card in a short period with one betting company. ‘There are triggers for harm data which would have flagged me up and they should have followed their duty of care, but rather than using it to signpost people to help and prevent them getting into trouble they use it to exploit them,’ she said.
Although gambling harm has traditionally been seen as a predominantly male issue, the number of women receiving treatment for problem gambling has doubled over the last five years to just under 2,500 according to GambleAware, while a Gambling Commission blogpost to mark International Women’s Day stated that almost half of women had gambled in the last four weeks when the National Lottery, scratchcards and bingo were included. Around a third of women aged 35-54 now gamble, with new analysis by NatCen and the University of Liverpool finding that ‘women who have online gambling accounts –for online slots, casino, bingo and instant win products – actually tend to play more often, for longer, and spend more than men’.
Describing the Sky Betting case, Gambling Commission chief executive Andrew Rhodes stated that, ‘Self-excluded customers are likely to be suffering gambling harm and should absolutely not be sent direct marketing that could tempt them back into gambling. We would advise all operators to learn from Sky Betting and Gaming’s costly errors and ensure their systems are robust enough to always prevent the self-excluded, and those who have clearly rejected marketing, from receiving promotional material. This latest fine would have been a lot higher had Sky Betting and Gaming allowed any of the self-excluded customers to actually gamble, failed to cooperate, and not taken decisive action aimed at preventing a repeat.’
NatCen/University of Liverpool: Exploring online patterns of play at www.begambleaware.org
In honour of International Women’s Day, Social Interest Group is this week running a series on the women of SIG.
Continuing with our IWD profile series. This is Tricia’s story.
When I sat down to speak with Tricia, I did not know that the interview would leave me humbled, emotional, thankful, filled with admiration, and most of all inspired! Tricia epitomises; perseverance, grit, determination, authenticity and most of all strength. This is her story.
Tricia
Synergy service manager Patricia Medford is a beloved colleague and friend, a mother of three and grandmother of five. Tricia as she is known, is a strong independent woman who has always had to fight for everything in life. “School wasn’t my best time, but I always knew there was something out there that was my passion. It just took me longer than others to find what it was. I’ve always had to fight for everything, nothing has ever been handed to me,” Tricia said.
Tricia’s current role was a light bulb moment for her. She had experienced a lot of domestic violence when she was younger and moved away from Luton with her children to make a fresh start. It took several years before she left that violent relationship and with her children, first moved to a refuge in Bedford then to Southend for a year. Tricia credits a conversation she had with a ‘church lady’ who picked them up in Southend, with showing her that her experiences could be used to help others. “I knew I had to give something back! She had given me and my children our lives back, so I knew I wanted to do that, to give back,” Tricia added.
Career
After a year or so in Southend, Tricia returned to Luton a different person. She found herself and was strong and independent. She was now a single parent so started courses at the Luton Learning center as well as doing English and Math. She then applied for voluntary work, which led to a job at the job center and learning center, supporting 16-to-25-year-olds to get back into education and employment.
Tricia then moved on to several different roles including working as a priority, prolific offender officer (PPO). Within that role, she worked alongside probation and the police dealing with predominantly housing and other support needs. This led to a job as a housing officer working with vulnerable people with complex needs. Because she’d had doors closed in her face as a youth, she knew what it was like on the other side and was determined to make a difference.
Then Penrose won the tender for the entire support services in Luton, so, Tricia was TUPE’d over and became a Penrose Employee, starting as a support worker. She loved it! She loved the interaction with clients and was a Gypsy Roman Traveler (GTR) specialist for a few years. Alongside this, she had a caseload of general complex vulnerabilities; all within sustaining and maintaining tenancies, early interventions, and prevention.
Tricia then successfully applied for the manager position and has been in this role for over 5 years, going from strength to strength. So, her career was great, but unfortunately, her health started to deteriorate. It started with a bad leg, which was attributed to sciatica. Then seemingly from nowhere, Tricia was diagnosed with bowel cancer at the end of December 2019.
The big C & SIG support
When she was diagnosed with cancer, it shook Tricia’s whole life. She had never really been ill before but went to the doctor to figure out a way to stop taking painkillers for her leg pain. The doctor examined her and told her that she had cancer. She didn’t believe him. That weekend she went to a Reggae festival in Manchester and didn’t tell anyone about it.
Then on Monday second December (a date she’ll never forget), she attended the hospital referral appointment. It wasn’t until she walked down that corridor and saw the Macmillan sign, that it really hit. She was checked, then taken into a room and gently told, (whilst having her hand stroked) her diagnosis – stage 4 bowel cancer! It was like a massive bombshell. Tricia had to be strong for her family and try to reassure them, telling them she was going to be OK. Although she didn’t know if she was going to be.
Turning Point’s Nat Travis discusses women accessing treatment services and how this could look post-Covid.
I’ve worked in the substance misuse sector for almost 20 years. During that time, we’ve seen new drug strategies come and go and the commissioning landscape change. Where we once had multiple providers working across geographical areas to provide a patchwork quilt of services for people (that were often hard to navigate and usually largely focused on drugs), we moved into an era of integrated community services often led by one provider.
Integration has, in my opinion, brought many benefits, including a wider range of services and seamless care coordination for people, but you could argue that some of the specialism has been lost in working with different cohorts and different needs, compounded of course by a decade of austerity. With the new drug strategy published in December 2021 and the funding commitment for the next three years, I am optimistic that as a sector we’ll be in a strong position to bring back specialism and support the needs of individuals in a more tailored way. But when I think of women in treatment, I’m not sure we ever had the specialism needed in the sector, with the exception of a few specialist organisations.
Traditionally, providers have always seen a greater proportion of males in treatment (often in the region of two thirds to one), so how do we change this and ensure that we provide the right opportunities for women to engage with treatment, and that our treatment offers them what they need?
The previous two years of the Covid pandemic have required us all to work differently, and many of the interventions we previously delivered face to face we realised we could deliver remotely. Something we have seen during this period at Turning Point is an increase of 25% in the number of females accessing treatment with us. Now we know that the needs of many people have increased during this difficult time, and overall, more people are accessing services, but the increase for us is weighted towards women, so does this different way of working encourage more women to access treatment?
Eleven of the country’s biggest treatment providers have joined forces to form the Women’s Treatment Group, which will work to improve treatment quality and options for women.
The group, which is chaired by Humankind, has already submitted a letter to the Office for Health Improvement and Disparities (OHID) outlining the minimum provision for women that should exist in every service.
Although the last decade has seen an almost 80 per cent increase in the number of women dying a drug-related death, the number of women seeking treatment has remained largely unchanged. The group will look at ways in which services could be adapted to better meet women’s needs, as well as recommending dedicated funding streams for women’s services and the creation of a ‘gender-specific’ evidence base.
All services should make sure there are women-only spaces and effective joint working with midwifery and local domestic abuse organisations, states the letter to OHID, alongside women-only trauma-informed group work and fully funded childcare provision. A key focus for the group will be working with parliamentarians to ensure the specific needs of women are fully understood, and it has already responded to the government’s Commissioning Quality Standard consultation stating that specialist women’s provision should be included in all service level agreements and that women’s lived experience needs to be fully valued.
Members of the group include Humankind executive director Karen Tyrell, CGL executive director Nic Adamson, Phoenix Futures CEO Karen Biggs, With You director Siobhan Peters, Trevi CEO Hannah Shead, Turning Point’s national head of service Natalie Travis and WDP CEO Anna Whitton.
Humankind executive director Karen Tyrell
‘Sadly, many treatment services can be an intimidating place for women and do not address the specific needs and challenges faced by women,’ said Tyrell. ‘Humankind and many of our partners do offer some services specifically for women but there needs to be a nationwide approach to ensure that irrespective of treatment type or geography every woman can get the help that they need. That is why we are calling on the government to allocate a portion of the new strategy funding specifically on women’s services and research into substance use treatment for women so that we can build a greater understanding of the needs of women and the most effective solutions to address them.’
A clear plan is needed to improve complex drug and alcohol services in Scotland, according to a report by Audit Scotland – the body tasked with making sure public money is spent effectively.
Drug-related deaths in the country are the highest in Europe and have been increasing for almost a decade, while alcohol deaths also rose steeply in 2020 (DDN, September 2021, page 4). Delivery of drug and alcohol services, however, remains complicated, with lines of accountability ‘not always clear’, the agency states. This makes spending difficult to track, including how the money is distributed and ‘what it is achieving’.
The Scottish Government has committed to spend £250m to tackle the country’s drug deaths crisis after years of falling investment, with £50m a year to be made available over five years (DDN, February 2021, page 4). However, details of how the money will be distributed across local areas have still not been published, says Audit Scotland. There were also persistent data gaps around referrals, waiting times and outcomes, alongside a ‘considerable time lag’ in public reporting. The range of organisations working across different sectors meant that clear accountability was needed from all partners.
Audit Scotland acknowledged that the government had provided additional investment for evidence-based treatments and establishment of the Drug Deaths Task Force, but said it was too early to assess their effectiveness.
Audit Scotland – Stephen Boyle.
‘We’ve recently seen more drive and leadership around drug and alcohol misuse from the Scottish Government,’ said auditor general Stephen Boyle. ‘But it’s still hard to see what impact policy is having on people living in the most deprived areas, where long-standing inequalities remain. Drug and alcohol data is not good enough, and there is a lack of transparency about how money is being spent and allocated. The Scottish Government needs to set out an integrated plan, with clear measures showing how extra spending is being used to reduce the tragic loss of life we’ve seen over the last decade.’
‘No one’ should be comfortable with what the report had to say, stated Scottish Drugs Forum CEO David Liddell. ‘We face huge challenges in Scotland with inter-related issues that demand a policy approach covering early years support to children and families, poverty, health, criminal justice and employability. What we have currently is confused.
SDF CEO David Liddell
Even with a narrow focus in the drugs field we have a recent strategy, Rights respect and recovery; we have the national mission [to reduce drug-related deaths] and later this year we will have the final report from the Drug Deaths Task Force with their own recommendations. As Audit Scotland recommends, there should be a process that shows how the aims and actions in these link together.’
There were far wider policy issues that related to problem drug use, he stressed. ‘Large numbers of people with a drug problem have been in care and have been parented by the state,’ which made delivery of the Scottish Government’s ‘the promise’ – to drive changes recommended by the Independent care review – a key element in preventing problematic drug use, while delivery of better outcomes in preventing and addressing homelessness was also crucial.
With death rates rising across services, Derbyshire Healthcare NHS Foundation Trust decided to dig a little deeper into the statistics. Martin Smith reports.
Around 2013-14, like many in the sector we began to see a rise in deaths within our services. As with other providers we were beginning to see a rise in all-cause mortality deaths, so we decided to take a closer look. Our task was to investigate the complexity of risk factors for premature all-cause mortality within the treatment population, and the impact of current clinical management.
There were 316 deaths of people engaged with Derbyshire Healthcare NHS Foundation Trust’s (DHCFT) substance misuse services – or up to one year post-discharge – between 1 January 2012 and 20 August 2020. The data cut-off point meant we only had a partial year for 2020 so it wasn’t included, but deaths in 2020 and 2021 exceeded those for 2019.
Overdose
Overdose (predominantly opiate) was by far the most common cause of death at 115 cases, constituting 40 per cent of deaths for which the cause was known. The cause of death was unascertainable or not yet known in 21 cases (7 per cent). After heroin or opiate toxicity, drugs such as diazepam, temazepam, gabapentin, mirtazapine and increasingly pregabalin were frequently highlighted under section 1b (‘underlying cause’ of the main cause of death) on the death certificate. All other deaths were physical health-related with the exception of suicides, of which there were 20 (6.3 per cent). The most common causes of physical health deaths were predominantly liver disease, COPD, bacterial infections and cancers.
The highest number of deaths occurred in the 35-39 age group, followed closely by the 40-44 age group. The age profile of overdose deaths followed the same pattern, but with a more pronounced peak in the 35-39 age group. The data suggests that those aged 50 and over are more likely to die from a physical health condition than an overdose – in the 50-plus age group 19 per cent of deaths were due to overdose, compared to 39 per cent of deaths in those aged 35-49.
When only chronic causes of deaths are analysed (brain-related illnesses, cancer, cardiovascular illness, diabetes, liver disease, lung conditions and kidney disease), the age profile becomes slightly older, with a peak in the 45-49-year age bracket. However, the data shows many deaths at a young age from these causes, with 58 per cent of deaths occurring in those aged under 50 and 22 per cent in those under 40.
The data shows that most individuals (161, or 52 per cent) were found alone, while 37 per cent (115) died in a hospital, hospice or care home. Most deaths in hospital were caused by physical health conditions – only 11 were due to overdose. Twenty-six of the people that died in hospital were receiving end of life care. Only 11 per cent of all decedents were known to have died in the presence of friends – of those people who were found alone, 80 per cent were male. Of the 115 people who died by overdose, an even greater proportion (72 per cent) were found alone. Ten per cent of overdose deaths occurred in hospital and 18 per cent in the presence of friends.
Physical health conditions
Physical health conditions were highly prevalent in the cohort that died, with 81 per cent of people (251) having at least one such condition – 60 per cent (186) had two or more. The most commonly occurring conditions were chronic obstructive pulmonary disease (COPD) at the time of death. In this study 243 decedents were under the age of 50. Of these 191 had at least one long-term health condition such as COPD, liver disease, or a heart condition, and 155 had an identifiable mental health condition, such as anxiety and depression disorders, personality disorder, PTSD or psychotic illness. Poor physical health and life-limiting conditions will continue to be a challenge to the sector. Three quarters of the people who died had also had at least one hospital admission in the previous 12 months – a significant red flag and a clear indicator of risk regardless of reason for hospital admission.
In addressing overdoses we started rolling out naloxone in 2015, and it’s likely that deaths both locally and nationally would have seen a greater increase without it. However, the prerequisite for naloxone effectiveness is that another person is present and available to administer it at the time of an overdose. With the number of people using drugs alone, living in isolation, and dying alone it is becoming clear that further interventions will be required, and it is highly likely that technology will play a key role.
Specialist Care
A partnership between Derbyshire Healthcare NHS Foundation Trust and ImpACT+, the specialist respiratory/COPD team based at the Royal Derby Hospital, was created to address a recognised need for access to specialist respiratory care for those using our services. This service is now delivered from within two of our treatment bases. More people have been diagnosed and commenced on treatment regimes, with one case of TB identified and treated. Many with symptoms but undiagnosed have been identified and received appropriate investigations for symptoms they had previously not addressed or been unable to access their GP to discuss. One client was identified to be suffering from a range of conditions including a DVT and heart failure and is only alive today because the health improvement nurse had access to the specialist team who were able to act accordingly on her concerns.
We continue to work in collaboration with several hepatitis C ODNs and peers alongside our nurses to eliminate hepatitis C – in the last two years only one person had hepatitis C referenced on their death certificate. We also introduced on-site ECG testing in Derby, with tests uploaded and results received within 30 minutes. A recent audit showed 33 per cent needed a follow-up referral, and the system is fully integrated with GPs, hospitals and our own data system. We will soon be rolling this out across the county. Future research should also examine the impact of opioid substitution treatment on mortality.
Engage and re-engage
In order to keep people engaged in treatment we employed an outreach worker to re-engage those who had dropped off their prescription and stopped attending appointments, and optimisation of medication is encouraged to allow people to find a dose that’s comfortable for them. More outreach workers were employed in the city and county to work specifically within the homeless community, and in the city we have an outreach worker to work specifically with females who are at risk.
Martin Smith is recovery lead at Derbyshire Healthcare Foundation Trust
One of the challenges the sector faces is not just deaths through overdose but deaths through physical health conditions. It sometimes appears that it is acceptable to talk about deaths in general but it’s still unusual to see services openly discuss all-cause mortality within their services. As we move into 2022 the full impact of COVID-19 on this client group is currently unknown, but it is reasonable to assume that the isolation and inequalities that they experienced pre-COVID would have intensified throughout 2020-22. As we all see a rise in the cost of living as always it is those with the least that will be most affected.
In Dame Carol Black’s influential Review of Drugs, she made a strong recommendation that treatment services should include people with lived experience of drug dependence working as recovery champions and recovery coaches. But she also warned that peer supporters should not be left to do the work of professionals without appropriate training, pay or support – an approach she described as exploitative.
A new guide co-produced under the leadership of Russell Webster in partnership with Revolving Doors sets out best practice in supporting peer volunteers derived from and informed by the lived experience of more than 250 peer volunteers. The guide covers a range of topics including training, support and helping people convert their volunteering experience into paid employment.
The guide can be downloaded here and you can also see a range of video interviews from commissioners, providers and people with lived experience on the accompanying website: https://peervols.russellwebster.com/
Read more in the forthcoming feature in April’s issue of DDN
As part of National Careers Week, Forward’s executive director of employment services Asi Panditharatna shares his reflections on the importance of green skills and careers in building the workforce of the future.
This week at The Forward Trust we are celebrating National Careers Week 2022. This year across Forward’s employment directorate we are focusing on supporting people to:
Take control of their careers
Explore and learn more about new opportunities
Dream big and aspire for a great career
Believe in themselves.
At Forward we believe that with the right support anyone is capable of bringing about and sustaining positive change in their lives.
Green skills and careers
Last year we started to teach green skills as part of our new Adult Education Budget programmes in London and Kent. We are now proud to be promoting an exciting range of Green Career Pathways, including apprenticeship roles in sustainability and jobs in sustainable construction.
As part of our green agenda, last month it was great to take part of the Association of Employment and Learning Providers Green Skills Summit. The summit outlined the green skills agenda and raised awareness of green issues. It focused on the practical steps needed to drive the demand for green skills from learners and employers. I was invited to be on the panel to discuss, ‘Are we ready to deliver the workforce of tomorrow?’ along with Simon Bozzoli from LDN Apprenticeships, Graham Duxbury from Groundwork and Patrick Craven from City and Guilds. The takeaways that stuck with me from the panel discussion were:
Green employment and jobs should be broadly defined so that learners and participants better understand the roles. For example, the International Labour Organisation (ILO) considers green employment to include activities such as community adaptation to climate change.
We know people want to make a positive difference through their employment. A global survey by Bath University found that 60% of young people are worried about climate change and want to do something about it. However, 70% of our learners from disadvantaged backgrounds say they have very limited knowledge of sustainability or awareness of the climate emergency. This can be compounded by preoccupation with other issues including unemployment or underemployment, poor housing, a lack of access to digital technology etc. As a sector we need to do more to make green skills and jobs equitable for all.
From day one, careers advice should be embedded into training so that learners or participants are aware of green job and apprenticeship opportunities. We know other organisations agree – the GLA Green Skills Adult Education Provision in London report supports this: ‘employers in all sectors felt that it was important to focus the adult education budget on developing long term career pathways for individuals with a broad range of skills, rather than short term jobs for particularly green tasks’. Better is possible. We are already working with Thames Water to offer apprenticeships and collaborating with other partners such as LDN apprenticeships to promote sustainable apprenticeships and employment.
Careers advice must be aspirational and help learners build the stepping-stones to realise their ambitions. In my experience, the base is set too low for people from disadvantaged groups. We can all do more to raise the bar.
Employers are critical to the success of skills and training programmes. On our programmes we offer opportunities for enrichment through employer involvement. This is a chance for employers to talk about their organisation’s missions and values and why they are keen to tackle the climate emergency. We encourage learners and participants to network with these employers, as well as offering opportunities for sector-based work academies, work experience, tasters and mentoring. We expect all our partner employers to align with the Good Work Standards and where possible be signed up to the Real Living Wage – giving people sustainable and equitable work opportunities.
In honour of International Women’s Day, Social Interest Group is this week running a series on the women of SIG.
We hope that you will enjoy these profiles and be inspired by them. Today’s feature is of our Clinical Lead, Muriel Gutu.
Muriel
What do you do when you have a high-stress job that requires integrity, accuracy, self-awareness, continuous professional development, people management skills, specialist knowledge, resilience, and diplomacy? Well, you ensure that the job does not become all-consuming or your entire focus, and you ensure that you balance the conflicting parts of your life. This is what our clinical lead Muriel Gutu does with dignity and grace.
Muriel is soft-spoken, charming, and direct. She laughs easily, even at herself. But there is an unmistakable core of steel running through her, forged through years of working in substance misuse and her Christian faith.
Muriel’s role has an organisation-wide remit, but her focus is on the CQC registered services
Muriel works with the clinical and medical teams and liaises with them on referrals. She is also responsible for clinical governance across the group, drafting, reviewing, and updating policies. To ensure the care we deliver is safe and within NICE guidelines, Muriel handles all clinical issues. She manages the process around controlled drugs and medication, carrying out regular audits to ensure accountability. She reviews incident reports, highlights lessons learned and ensures their dissemination. Muriel also provides in-house training and supervision to nurses and leads in their recruitment.
Career and challenges faced
Muriel’s nursing career started many years ago. She initially worked in acute mental health and as a community psychiatric nurse, then focused on substance misuse. She worked in community settings with drug and alcohol teams within the NHS, working as a locum and in prisons.
Muriel qualified as a nurse prescriber in 2008, which entails prescribing medication and carrying out clinical diagnostics in substance misuse. The course is an intense one, and Muriel did it alongside working full-time with young children. She was discouraged by others due to the intensity of the course and the commitment needed. Many people are discouraged from pursuing it or shy away from the responsibility. Sometimes nurses are qualified as prescribers but don’t prescribe. Muriel credits her stubborn nature for seeing it through and qualifying. She worked as a nurse prescriber in different settings within the community and held various managerial posts.
Muriel faced various challenges working as a nurse prescriber as a woman of colour. She sensed resistance from some non-prescribers and clients who sometimes did not understand how she could prescribe their medication. Because they are used to women as nurses and doctors doing the prescribing. This reflects the views held by some of society today. She also faced resistance from some medics, but thankfully, there is now a general understanding that doctors and prescribers can complement each other. Sometimes, Muriel worked with and supported Locum doctors who had limited substance misuse experience.
Muriel overcame her challenges by showing confidence and demonstrating competence. She escalated anything that felt like a racial attack and quickly moved on, determined that these incidents would not define her or lower her self-esteem. Muriel eventually left the NHS out of frustration after being overlooked for a promotion.
Muriel prescribed mainly in the third sector and leant on the prescribers’ forum for support and regular updates on new medications and practices. Prescribers need to be supervised and mentored by a doctor and insured against malpractice, offering some reassurance.
Muriel joined Brook Drive as a Locum Nurse Team Leader in 2019. Prescribing was not part of the role as this wasn’t part of the Brook Drive set-up. After one year, when the post became available, she was appointed Clinical Lead in recognition of the to work she had done since joining SIG.
Muriel found working at Brook Drive a fantastic experience as she was part of a team. Her work for the group is mainly positive, although it was initially isolating as she did not feel part of the established Heads of Service group. That has changed, and she is utilising her skills much more, liaising with services on the unifying aspects of medication management and mental health and interacting with Heads of Service working for the wellbeing of Service Users.
Muriel thinks that a health strategy for the organisation is needed. She is working towards creating enhanced policies and processes in general health, diabetes, obesity management and smoking.
Just as lockdowns saw drinking shift from physical venues to home, so it was with gambling. But the exponential rise in online gambling – where anyone with a smartphone has instant access to a vast casino that never shuts – is hitting women particularly hard. DDN reports.
Read the full article in March DDN
The hearing into the role gambling played in the death of 24-year-old Jack Ritchie has once again put gambling addiction in the headlines, and coincides with the NHS informing the GambleAware charity that it would no longer be accepting funding from the industry for its gambling clinics (see news, page 5 ). Ritchie had started gambling while at school, using his dinner money to play on fixed-odds betting terminals (FOBT), dubbed the ‘crack cocaine of gambling’. Just seven years later he took his own life, with his parents arguing that he was addicted to ‘products licensed by the start’.
Last month NHS mental health director Claire Murdoch wrote to GambleAware confirming that the NHS will fully fund its own gambling services from April onwards, following unease among clinicians and patients around the perceived conflict of interest of industry funding for treatment. May will see the NHS open two new gambling clinics, in Southampton and Stoke-on-Trent, to complement its existing services in Leeds, London, Manchester and Sunderland, as well as the national children and young person’s clinic.
The two new facilities are to help meet the ‘record demand for specialist support for gambling addiction’, the NHS states, with rates of online gambling in particular rising over the last couple of years, as people worked from home or found themselves with huge amounts of time on their hands after being furloughed. A study led by the University of Bristol found that, while lockdowns meant that overall people were gambling less frequently as physical premises closed their doors, use of online poker, bingo and casino games increased six-fold among people who were already regular gamblers.
Online games have also made gambling much more accessible to women, who may have been unlikely to visit high-street betting shops. A YouGov poll of almost 10,000 women using the Problem Gambling Severity Index found that up to 1m women may now be at risk of gambling harm, and according to GambleAware the number of women receiving treatment for problem gambling has doubled over the last five years to just under 2,500 – a figure that’s likely to represent ‘a fraction’ of those experiencing gambling-related harms, the charity states. Just under 40 per cent of women may also ‘refrain from seeking help or treatment’ as a result of the stigma surrounding the issue, with GambleAware launching its first harm prevention scheme aimed specifically at women earlier this year.
‘Gambling behaviours manifest themselves differently in women than men,’ said gambling addiction counsellor Liz Karter. ‘For example, we know the easy availability of online gambling leads many women to games which appear innocent and socially acceptable. The games seem safe and familiar, as they are so similar to the free play digital games we are all now used to playing. In addition, the hopes of financial gains can prove a powerful motivator. While gambling doesn’t always lead to harm, it’s vital women are aware of early warning signs including losing track of time, incurring increasing debt, or a tendency to hide gambling from others or gambling to forget their problems.’
As almost all literature on gambling harms has so far focused on men, GambleAware has commissioned IFF Research, the University of Bristol and GamCare’s Women’s Programme to carry out a three-phase research project, Building knowledge of women’s lived experience of gambling and gambling harms across Great Britain, which will run until the end of this year. The project will explore why women take part in different types of gambling, the effect on their lives, and their experiences of treatment and support.
‘We conducted a rapid evidence assessment which found that much of the academic research on gambling has long focused on men, or assumes that only men may develop problems with gambling,’ said Prof Maria Fannin of the University of Bristol. ‘This is starting to change as we learn more from women themselves and their experiences. We want to know more about how gambling becomes part of women’s lives and how their experiences may differ from men’s. Ultimately, we want our work to change the public perception and awareness of who can develop problems with gambling and ensure women’s needs and concerns are taken into account.’
Kelly’s story
The intimidating men-only environments of betting shops meant that problem gambling was largely a male problem, but the rise of online gambling has changed all that.
Kelly Field describes how what started as a few games of online bingo led to financial and emotional devastation.
I started with online bingo sites in around 2012. I was looking for an escape from reality, and you’ll find that with a lot of women you speak to – they want escapism from day-to-day life or from trauma. I think I realised I had a problem early on, but you cross that invisible line of it becoming an addiction.
Within six months I’d spend ten and a half grand on one credit card, no questions asked. There are triggers for harm data which would have flagged me up and they should have followed their duty of care, but rather than using it to signpost people to help and prevent them getting into trouble they use it to exploit them. The credit card company didn’t say anything either, and it’s taken me seven years to pay the debt off. But I spent a lot more than that overall.
You sort of know you’ve got a problem, but you think “I’ll win the jackpot and pay it back and I’ll be alright.” You have these delusional thoughts of “everyone’s a winner”, because that’s how it’s portrayed. A lot of people assume it’s just a financial issue but it’s not just money you lose – it’s self-worth, self-esteem, self-confidence. My mental health was at rock bottom and I put on loads of weight because I just isolated myself in the house playing these games. My son didn’t get the things he wanted, we didn’t go on holiday. There were times when we had £20 a week to live on. You lose more than money.
People have this stigma and embarrassment, and they’re not telling anybody. They’ve got all this debt and can’t tell people how they got it and it causes people to take their own lives, because they’d have to admit they’ve got a gambling addiction. I became suicidal – you get in such a dark place with it and it just consumes your whole life. It takes over and you think the only way out is to end your life, because then it’ll stop.
At the time there were very few support services. There was basically only Gamblers Anonymous, but I’d never have gone to that as a woman because it’s a completely male-dominated environment. The lived experience people who work for the services and charities now are still predominantly men, so when they go into schools and colleges speaking to young people it just reinforces that message that it’s still a male-dominated addiction. But you can see how women are targeted in the daytime with the pink and fluffy bingo adverts and then in the evening it’s all casinos and football – they know exactly what they’re doing. Every other advert is a gambling advert, and they’re using celebrities to endorse it. You couldn’t put adverts for pornography on TV because there’d be uproar, but the gambling advertising on TV and social media normalises it for young people – these are adult products.
The point I knew I needed treatment was when I’d maxed out all the credit cards but I managed to get a £1,600 overdraft on our joint account, and within 50 minutes I’d spent all of it on slots online. I was devastated and disgusted and ashamed, and I had to ring my partner and tell him I’d done it again after promising to stop so many times. I just snapped the card up and started cutting at my wrists. The GP gave me pills and got me a counselling appointment but the counsellor didn’t turn up the first time so I never went back. I carried on gambling for about another 18 months before I found a local service and got a 12-week talking therapy.
I’ve tried to turn a negative into a positive and I’ve campaigned to get credit cards banned for gambling and to raise awareness of gambling addiction, particularly with women. I relapsed once early on but I’ve got [blocking software] Gamban on my phone and I stay away from all forms of gambling. It would be like an alcoholic saying they’ll just have one drink – it would soon be a bottle of vodka. In some ways gambling addiction is easier to hide than with drugs or alcohol, because there’s no substance. You can be in all this debt and about to lose your family and your home but you can put a smile on your face and no one will know. But we have far, far too many suicides that are directly linked to gambling addiction.
Looking for an escape from reality drew Kelly into online bingo – a few games that led to an all-consuming gambling addiction and financial and emotional devastation (page 6). This addiction may be ‘invisible’ but the drivers can have much in common with any other form of compulsive behaviour that offers us time away from real life.
‘For many people addiction is a response to trauma that has not been dealt with,’ Alice Wiseman reminds us (page 18) as she shares a public health perspective that feels like an opportunity to collaborate far more actively with our healthcare partners. We’ve grasped the need for ‘trauma-informed’ care – but just look at the outcomes we could achieve if we focused our attention in a really robust way on reducing ACEs, as she suggests, changing the narrative from punishing and criminalising to understanding the causes of behaviour.
Looking for the reason for tragedies never makes for easy reading, but The Suicide Prevention Consortium’s research on alcohol-related suicidal behaviour (page 16) and Martin Smith’s look at causes of drug-related deaths (page 14) are two articles that could have an important role in informing our actions.
‘My greatest worry about my review and its potential is can we deliver it at the local level,’ Professor Dame Carol Black told the Westminster Social Policy Forum’s Tackling drug dependence and improving delivery of services seminar.
‘We’ve acquired the investment – that was of course crucial, but there must be much greater accountability for the spend.’
The Treasury fully intended to ‘hold us to account’, she stated, echoing warnings from others in the field (DDN, February, page 8). Local authorities would need to work with wider health, employment, housing support, criminal justice and social care, and develop joint commissioning plans and joint needs assessments. Years of austerity had meant that the idea of creating a whole systems-approach ‘wasn’t able to happen’, she said, ‘and what I’m hoping from my review is that we’ll now be able to do that, because it’s absolutely needed.’ This would require at least six departments of state to be ‘truly and sustainably involved’, she said. While it ‘wasn’t that they hadn’t been interested before’, competing priorities meant that it had always been low on their agenda.
All but one of the 32 recommendations in her Review of drugs: phase two report had been taken on board in the government’s new drug strategy, which was ‘very pleasing’ – and accompanied by a financial settlement that was ‘probably 70 per cent of what I’d asked for in the original part two review’ and ‘very big’ ambition. ‘But I don’t want, now that we’ve got more money, to just do more of the same,’ she stated. ‘This is a unique opportunity to really think about what does a very good treatment and recovery service look like.’
Starting from a low base
It was important to be aware that in some places ‘we’re starting from a low base, and we’ll need to support and enable improvement in some of our local areas,’ she said. The sector was facing a challenging journey, not least in terms of re-building the workforce. ‘That’s going to require a really sustained focus – we can’t just do it overnight.’ Similarly, research had been ‘bottom of the pile’ in almost every aspect of addiction, with a corresponding lack of financial support.
Workforce was a ‘critical challenge’, agreed head of inclusion at Midlands Partnership NHS Foundation Trust, Danny Hames. There was promising evidence of positive cross-sector working, but providers needed to be ‘brave and a bit humble’, he said. ‘We need to open ourselves up to accountability and be transparent, but we also need to be sure we’re working in the best interests of patients. Collaboration is absolutely key.’
Moving forward
‘We’re at the point where we have to look at the competence of our own clinical practices and commissioning process so we can move the field forward,’ said head of King’s College London’s National Addiction Centre, Professor Sir John Strang. One of the major challenges would be improving the quality – as well as the quantity – of treatment, and there was a significant challenge around training need. ‘We need to look at how to support and improve the development of the general workforce, so that somebody entering treatment is being seen by someone with a good, broad knowledge of the treatment field and how to integrate medical and social interventions,’ along with developing a cadre of specialists for the future.
From a research point of view, what was needed was a serious commitment to a much more practice and policy-orientated research agenda, he said. ‘If you look at the National Institute on Drug Abuse in the US, we don’t have anything comparable – which means we don’t have that critical science perspective.’
While the strategy committed to building a world-leading evidence base there was no mention of consumption rooms, said Release executive director Niamh Eastwood, despite evidence of their effectiveness and ability to provide access to treatment and other support. The strategy was a ‘tale of two competing directions’, with ‘once again an over-focus on criminal justice responses’ – something that undermined the ambition to get people into treatment. ‘When we treat people first and foremost as criminals, it’s very hard to address their health needs.’
The evidence base
‘We’re traditionally seen as the enforcers,’ deputy chief constable of Lincolnshire Police, Jason Harwin, told the seminar. ‘And let’s be very clear, we have significant numbers of serious organised criminals who are exploiting young and vulnerable people, who we have to continue to enforce the law against. But we do need to make sure we’re diverting individuals to effective, evidence-based treatment services that we know reduces their vulnerability and their likelihood to continue to commit offences.’
‘From my own experience of addiction I’ve lived a definition of madness, which is doing the same thing over and over again and expecting a different result,’ said the Scottish Recovery Consortium’s lived experience officer, Michaela Jones. ‘The only solution in these circumstances is to stop and recognise the need for radical and sustained change – in this case it’s to accept that the resilience and flexibility of the drugs market make it almost impervious to enforcement activity.’
There had in fact been extensive, informal decriminalisation, said Strang. ‘It’s not been driven by laws, it’s driven by changing attitudes within different police forces and within society, and that’s a much more important level at which to engage.’
Deprivation
In terms of preventing dependency, Release had consistently argued for re-allocating some of the ‘endless resources’ for law enforcement into trauma-informed counselling in schools from an early age, said Eastwood. ‘We know adverse childhood experiences are one of the biggest drivers for drug dependency. That could have a massive impact – addiction isn’t all about the drugs, it’s very much a response to abuse, neglect, deprivation.’
Market forces
Legal and illegal drug markets went ‘back and forth’, said Dr Keith Humphreys, professor of psychiatry at Stanford University, advisor to the Carol Black review and former drug policy advisor to President Obama. ‘It was legal companies that flooded our healthcare system with a 400 per cent increase in per capita prescribing, and many, many people got addicted to those drugs. Heroin traffickers then realised “there’s gold in them thar hills”, started to expand to different cities and began getting as customers people who were addicted to legal drugs like oxycontin.
‘If you believe that full legalisation, as is commonly said, will only bring good things then you have to be candid about what we’ve learned about the legal drugs we have’, he continued, as tobacco and alcohol killed far more than all illegal drugs combined. ‘If you’re going to argue – as many bright people have – that we should have corporations like the tobacco industry sell methamphetamine and cocaine, you should explain why those drugs wouldn’t then be up there at the top of that list.’
Reducing demand
In terms of reducing demand, while it was possible to use the media to encourage people to access services or give them factual information, advertising campaigns to discourage drug use simply didn’t work, he said. ‘Demand responds to supply, as is well demonstrated across all kinds of industries. Within the prescription system, where we at least putatively have a huge amount of control, if we don’t exercise that wisely we’ll get a lot more demand as we’ll make many more people dependent on – in the US and Canada – opioids, but also benzodiazepines, stimulant medication and so on.’
Ultimately, putting the person at the centre of services was vital, stressed Black. ‘We would do that with any other condition, and this really is a chronic disease with remissions and relapses. The real issue for me now is how do we keep this energy up, and enable it to go forward, keeping the government’s foot on the peddle and making sure it really is a whole-systems approach. We really have the opportunity to improve a quite dire situation when it comes to treatment and recovery. There’s a willingness to think about doing things differently. But everyone also recognises the hill that needs to be climbed.’
Landmark opportunity
‘This is a landmark opportunity for a system transformation that will help us save lives and improve outcomes for individuals and the communities in which they live,’ said Rosanna O’Connor, director of addictions and inclusion at the Office for Health Improvement and Disparities (OHID). ‘It’s a very significant moment.’ It was also important to put aside concerns about the criminal justice focus, she said. ‘It’s through the criminal justice lens that we’ve landed ourselves such significant investment in treatment and recovery.
‘It’s surprising to find myself on a platform saying the politicians have delivered, and it’s now in our hands as a sector. We have to collaborate to deliver, and really up our game across the whole system if we’re to have any chance of having this investment sustained. We can do it, but we have to do it together.’
Why are widespread libertarian views on issues like vaccine passports usually at odds with the same people’s opinions on drug prohibition, asks Nick Goldstein.
Nick Goldstein is a service user
Just when you thought it was safe to read DDN again… I’m back! Harm reduction is as much a chronic relapsing condition as addiction, and after being hopelessly involved in harm reduction for far too long I’d decided I deserved a sabbatical, maybe even a permanent vacation.
So, I’m on sabbatical/vacation minding my own business and everything is tickety boo, but early in 2021 I started to feel uneasy. Something was bugging me and I couldn’t figure out what. This seemed more than your average pandemic blues, and I noticed the unease intensified whenever I watched the news or read a newspaper. Everyone feels mildly nauseous while watching the news these days, so I put it down to general anxiety. But this felt different.
Epiphany and diagnosis finally came while watching the Beeb’s one o’clock news with, of all people, Andrew Bridgen MP discussing public health laws in the form of vaccine passports, which he harrumphed were ‘a major infringement of civil liberties!’ I was fairly amazed by his attitude, as anyone who’s been arrested, charged or even imprisoned for breaking another of those public health laws, like, I don’t know, a drugs offence perhaps would be.
Ironically, I remember, back in the day, meeting my old friend Jimmy on his way to court. I asked how he thought it would go and he replied ‘nothing good’s going to happen. Whatever happens my civil liberties will be flouted’. He was joking, but the judge saw it differently and told him so – while flouting his civil liberties. This was long before Mr Bridgen saw the light, so no one was there to question the court’s approach to civil liberties and public health.
Public health laws are government, at various levels, trying to improve the health of the general public with policy and legislation involving environmental health, community health and epidemiology, among others. Public health laws are never popular because they amount to a blunt tool that inevitably limits behaviour, but up until recently they were accepted as necessary for the greater good. Public health laws have been introduced for a wide range of issues ranging from tobacco and alcohol use to zoning and quarantine laws and, of course, drug prohibition, employing policy tools from taxation to criminalisation.
No one likes being fined or jailed, but public health laws and the penalties they engendered were accepted as necessary – the price we all paid to be part of a society. That was until recently. You see Mr Bridgen’s not alone in his re-evaluation of the relationship between the state and the individual, and its impact on public health. Mr Bridgen is just one of what appears to be a growing group of people with a very libertarian take on events – a whopping 126 MPs voted against the public health legislation around vaccine passports. MPs across the political spectrum voted against enacting a law the primary aim of which was the protection of their constituents’ health – ranging from Jeremy Corbyn (natch) to Sir Graham Brady to Caroline Lucas. They were cheered on by a large section of society, from hardcore anti-vaxxers to lapsed Nazis to aged socialists all protesting public health laws as infringements that compromise their liberties.
None of these people seem to have considered how their attitudes to public health might impact other areas – like drug prohibition. I mean, we have laws to protect everyone’s health. You can’t claim that one deadly disease should be prohibited and punished with criminalisation and then claim another should be ignored because action infringes your liberties. It’s simple, we either believe in protecting society or we place an individual’s rights before all else. It appears that a little consistency in our elected representatives’ attitudes to public health laws is asking too much.
I guess on the plus side that inconsiderate comments from our political masters regarding the iniquity of public health laws and primacy of civil liberties reveal a sea change in attitudes to the ethos of the state and the individual – or to put it another way, you can’t talk shit about rights without it impacting on other areas of public health policy, like substance misuse treatment. With a little luck this change of attitude and growth of libertarianism might spark a wider discussion on civil liberties and public health laws. Well, I feel a lot better for working out what was bugging me. Now… back to my sabbatical.
Dame Carol Black has visited WDP’s residential detox and rehabilitation facility Passmores House to meet with its IPS (Individual Placement and Support) Into Work team.
Following the release of WDP’s IPS Into Work Impact Report, Dame Carol Black will be meeting with its service users, IPS Into Work team and Kim Archer, West London Alliance commissioner, to hear more about the success of the innovative employment support scheme.
In Dame Carol Black’s second part of her independent review on drugs, she identified employment as being an ‘essential part of recovery’ and called for the roll out of IPS services across England.
Since early 2019, WDP’s award-winning IPS Into Work service has focused on achieving sustainable employment to help reduce stigma, enrich lives, boost local economies, develop additional talents, and create workforces that reflect the diversity of their local communities.
Despite a challenging year due to the pandemic, WDP’s IPS Into Work team has supported 218 service users into employment and provided over3,700 hoursof support to participants during 2019-2021.
Yasmin Batliwala, chair of WDP, sai, “We are delighted to welcome Dame Carol Black to Passmores House today to meet the IPS team following the release of our IPS Into Work Impact Report. The report demonstrates how innovative employment support can transform the lives of people in recovery and we are proud to showcase the excellent outcomes and activities delivered by our teams.”
Kim Archer, West London Alliance commissioner, said: “It is a pleasure to meet Dame Carol Black, and to have worked with WDP to help people with addiction to maintain their recovery and rediscover the opportunities and self confidence that employment brings. I am delighted that the West London Alliance was at the forefront of expanding IPS to this group of people.”
Alcohol-related deaths in Scotland increased during the pandemic despite lower drinks sales, according to analysis by Public Health Scotland (PHS). While rates of alcohol-related hospital stays fell, the increase in deaths was driven by people aged 45-64, mostly men – ‘groups that experienced the highest rates of deaths caused by alcohol prior to the pandemic’.
Men aged 45-64 feature in the analysis
The analysis is based on data for alcohol sales up to May 2021, hospital stays to March 2021 and deaths to December 2020. The increase in deaths is despite sales for 2021 being almost 10 per cent lower than the 2017-19 average, and 16 per cent lower for the January-May period. Despite the overall fall in sales during the pandemic, population-level consumption was still above recommended levels, says PHS, with 17 units of pure alcohol per adult sold every week, representing enough to ‘put every adult in Scotland over the chief medical officer’s low-risk weekly drinking guideline’.
The findings echo previous studies for the UK as a whole which found that while some people cut their drinking during the pandemic, many who were already drinking at hazardous and harmful levels increased their consumption. Scotland’s rate of alcohol-specific deaths for 2020 was 22 per 100,000 population, says PHS, 8 per cent up on the average for 2017 to 2019 and ‘higher than any individual annual rate in the study period.’ Deaths rose by almost a fifth between 2019 and 2020 (DDN, September 2021, page 4), following a decline the previous year, prompting campaigners to call for the minimum unit price to be increased to 65p (https://www.drinkanddrugsnews.com/increase-minimum-price-to-65p-scottish-government-urged/).
Lucie Giles: Tackling alcohol harms among high-risk groups should be a critical objective
‘The data show that the number of people accessing hospital with an alcohol-related diagnosis fell during the pandemic, particularly at times when restrictions were at their most stringent,’ said public health intelligence principal at Public Health Scotland, Lucie Giles. ‘We saw the greatest reductions amongst men and those aged 45 years and over and it was in these same groups that we saw increases in deaths caused by alcohol. This was despite average alcohol consumption for the population falling, a change driven by a reduction in sales of alcohol through pubs and clubs.
‘Taken together, the evidence points to increased drinking amongst some groups, coupled with a reduction in the number of people accessing hospital treatment and greater rates of death caused by alcohol,’ she continued. ‘Tackling alcohol consumption and harms, particularly among high-risk groups, should be a critical objective of any COVID-19 recovery plans.’
Alcohol sales and harm in Scotland during the COVID-19 pandemic at www.publichealthscotland.scot – read it here
The NHS is set to open two new gambling clinics, it has announced, following ‘record demand’ for specialist support. The clinics, in Southampton and Stoke-On-Trent, will open in May and take the number of NHS specialist gambling services to seven. Almost 700 people with the ‘most severe gambling addiction issues’ were referred to NHS support between April and December last year, a 16 per cent increase on the previous year.
The DDN guide on gambling addiction helps identify problems and the available treatment options.
The pandemic has seen a huge increase in the number of people gambling online, with the closure of betting shops during lockdowns and the widespread shift towards working from home. Almost 625,000 more over-65s are also now gambling online at least once a month than before the pandemic, according to analysis by the Royal College of Psychiatrists (https://www.drinkanddrugsnews.com/pandemic-responsible-for-huge-increase-in-over-65s-gambling-online/).
Research published by Public Health England (PHE) in 2021 estimated that almost 250,000 people were likely to have some form of gambling addiction, with around 2.2m classed as ‘at risk of addiction’. PHE’s evidence review into gambling harms estimated the annual cost to England alone at more than £1.2bn, almost £620m of which was ‘an estimate of the economic cost of gambling-related suicide’ (https://www.drinkanddrugsnews.com/cost-of-gambling-harms-at-least-1-27bn-a-year/).
Claire Murdoch: ‘Gambling addiction is a cruel mental health condition.’
The announcement of the new clinics comes as the NHS has written to GambleAware stating that it will be ‘fully funding its own gambling services’ from April, following concerns about conflicts of interest around the industry’s funding of treatment.
‘Gambling addiction is a cruel mental health condition that can devastate people’s lives – our pilot clinics are already having a lasting impact in helping people to take back vital control of their lives,’ said NHS mental health director Claire Murdoch. ‘The opening of two new gambling clinics in May, as a part of our £2.3bn investment into mental health services, will mean we can help even more people with the most serious gambling problems. Later this year the NHS will launch a new Gambling Harm Network and Clinical Reference Group, which will bring expertise together and enable clinical teams to share best practices for helping to treat gambling addiction.’
This LGBTQ+ History Month, drug and alcohol practitioner Darren Lacey explains why he set up a dedicated LGBTQ+ recovery group at The Forward Trust.
Hey I’m Darren, a drug and alcohol practitioner at the Forward Trust. I’m 43 years old and a (now) proud gay man…
It wasn’t always that way. I used to feel shame, guilt, angst… the list of negative emotions is endless. I knew from primary school age that I was different. I was born in 1978 so witnessed the AIDS crisis of the 1980s as a child. It scared the hell out of me – who can forget those horrific adverts?!
I bore the brunt of Section 28 – which banned ‘the promotion of homosexuality’, meaning if I was to go to a teacher and tell them I thought I was gay, they were not allowed to talk to me in any way about it, it could have meant them losing their job. My experience of this institutionalised homophobia is something I would later understand to have had a hugely negative impact on my life: my mental health, my sense of identity and belonging, contributing to my experience of addiction and then recovery.
On the 18 February this year I celebrated three years sober. In those three years I’ve learnt so much about myself – mainly about my sexuality and to be proud of who I am. I was lucky enough to get support with my own addiction, completing a community detox through The Forward Trust (Forward). I found out more about myself in those 13 weeks than the past 40 years.
About 18 months into my recovery I was asked to speak at an online recovery meeting. As someone who doesn’t attend Fellowship meetings, though I know this is key to many people’s recovery, I wasn’t used to speaking to a large group and I was really nervous, but I had learnt to speak my truth.
I went to the meeting and bared my soul. It was an amazing experience, I found it really cathartic. I spoke about things I struggled with as a kid and things I was still trying to work on. I spoke about what I later learned to describe as my ‘internalised homophobia’. I spoke about self-loathing, guilt, shame, the battle between my masculine and feminine sides… all these things I thought were unique to me. Within an hour, I had received messages of love and support which, in all honesty, was quite overwhelming. These people seemed to like me and understand my experience. How?! I wasn’t even sure I liked me!
One of these messages was from the meeting host who said so much of what I talked about had resonated with him and that even he felt he was alone in those thoughts. We chatted on Twitter for a bit and came up with an idea to host an LGBTQ+ recovery meeting. So we did it…
In the first meeting we had people from all corners of the globe – UK, Canada, USA, New Zealand, Ireland… Whaaaat!? It was incredibly inspiring. We shared common experiences and struggles around how a lack of acceptance in society and in ourselves was a leading cause for our addictions. I started researching the relationship between addictions and the health of the LGBTQ+ community and was shocked, yet not surprised, about what I learned.
We know that drug and alcohol use among LGBTQ+ groups is higher than among their heterosexual counterparts, irrespective of gender or age. As a community, LGBTQ+ people are at a higher risk of experiencing mental health problems than the general population. I wanted to do something about it.
Police officers across the whole of Scotland are to be equipped with and trained in the use of naloxone, Police Scotland has confirmed.
Pilot schemes were carried out in in Falkirk as well as Caithness, Dundee, Glasgow and Stirling.
The national roll-out follows pilot schemes in Caithness, Dundee, Falkirk, Glasgow and Stirling that saw more than 800 officers trained to use naloxone and more than 650 volunteer to carry nasal spray kits.
All operational officers across the country will now carry naloxone spray, says chief constable Iain Livingstone, following an independent review last year by the Scottish Institute for Police Research which recommended a national roll-out. Work has already commenced to ensure there are sufficient stocks of naloxone to equip more than 12,000 police, along with a national training programme. The roll-out extends to all officers in response and community roles, along with armed police, dog handlers, public order and road police up to the rank of inspector. Any other officers or staff are also free to undertake the training, says Police Scotland.
Scotland’s drug death rate has long been by far the worst in Europe, and remains three and a half times greater than the UK as a whole. There were more than 1,300 drug-related deaths in Scotland in 2020, and while provisional figures for 2021 show a slight decrease these are taken from initial police reports rather than the official statistics from National Records of Scotland, which are based on death certificates and pathologist reports.
Chief constable Iain Livingstone
‘I know the terrible toll of drugs deaths in Scotland and policing is committed to playing our part in reducing the harm caused to individuals, families and communities,’ said Livingstone. While preventing drugs from reaching the streets and bringing organised criminals to justice would remain a key priority, preservation of life and keeping people safe ‘lies right at the heart of policing’, he said. ‘We have a purpose and remit which goes beyond law enforcement. We have a positive legal duty to improve the lives of our communities. Equipping and training officers with naloxone will contribute to that mission. Where a person is suffering an overdose, naloxone nasal spray can be given safely by officers with no adverse effects.’
SDF strategy co-ordinator for drug death prevention, Kirsten Horsburgh
It was also crucial that ‘timely and sustainable support is available to provide treatment for those suffering addiction’, he stated. ‘I’m grateful to all the officers who stepped forward during the trial to carry naloxone and help their fellow citizens when they needed it.’
‘Police officers are often first on the scene of a suspected overdose and are well-placed to act quickly and potentially save a life – the pilot has shown this,’ added the Scottish Drug Forum’s strategy co-ordinator for drug death prevention, Kirsten Horsburgh. ‘Expanding naloxone carriage by police to cover the whole of Scotland is significant, and an obvious next step. It has been positive to hear frontline police recognising that this is part of key policing duties to preserve life, and be able to intervene effectively.’
‘Woefully inadequate’ labelling is keeping consumers in the dark about the sugar and calorie content of their drinks, according to new analysis commissioned by the Alcohol Health Alliance (AHA).
Just 20 per cent of the labels displayed the wine’s calorie content.
It was possible to consume almost the entire recommended daily limit of sugar from two medium-sized glasses of popular wines, the researchers state.
The study involved analysis of 30 bottles of leading-brand red, white, rosé, fruit and sparkling wines, none of which displayed sugar content on their labels, despite this being a requirement for non-alcoholic drinks. Just 20 per cent of the labels, meanwhile, displayed the wine’s calorie content. A 175ml glass of Barefoot Bubbly Pink Moscato was found to contain 13.8g of sugar, almost half of the government’s 30g a day guideline, while bottles of Yellow Tail Shiraz, Hardy Stamp Shiraz Cabernet, Campo Viejo Rioja Tempranillo and Casillero Del Diablo Cabernet Sauvignon all contained close to 600 calories each.
‘Alcohol is very energy dense, with just two medium-sized glasses of the most calorific wines analysed containing more calories than a McDonald’s hamburger,’ says AHA. However people who wanted to know the calorie content of their drinks would have no way of knowing in most cases, with AHA describing alcohol’s exemption from food and drink labelling regulation as ‘absurd’. Previous YouGov surveys have found that more than 60 per cent of people wanted calorie information included on alcohol labelling, with more than half wanting sugar content. The government promised to consult on calorie labelling for alcohol as part of its obesity strategy to ‘beat coronavirus and protect the NHS’ (DDN, September 2020, page 4), the results of which should be published ‘without delay’, says AHA.
Dr Richard Piper is CEO of Alcohol Change UK
‘This study, along with so many others, reveals a huge failing in alcohol labelling,’ said Alcohol Change UK chief executive Dr Richard Piper.‘We as consumers have a right to know what’s in the food and drink we consume and the effects it could have on our health. But time and again we uncover evidence of a woeful lack of even the most basic information on alcohol labelling. As shown by this study, the huge variation and lack of correlation between sugar and alcohol content in wines means that consumers have no way to even infer how much sugar they might be consuming. It’s totally unacceptable that so many alcohol labels continue to fail to display vital health information such as calories, ingredients or nutritional information, as well as the number of units in the bottle or a serving, and the chief medical officer’s low-risk drinking guidelines.’
The Home Affairs Committee is to investigate the impact of legislation designed to restrict drug use, including the Misuse of Drugs Act 1971 and Psychoactive Substances Act 2016, it has announced. The investigation will form part of a wider inquiry to ‘examine illegal drug use in the UK and its effect on society’.
The Misuse of Drugs Act’s 50th anniversary last year saw it labelled ‘past its sell-by date’ and ‘not fit for purpose’ (https://www.drinkanddrugsnews.com/experts-call-for-drug-law-reform/), while the 2016 act was also highly controversial. The inquiry also intends to look at the effectiveness of government strategies to address drug use and drug-related deaths and crime, including the new ten-year strategy launched late last year. Questions the committee will consider as part of the inquiry include whether the current framework needs to be reformed, should a ‘right to recovery’ be enshrined in UK law, and which international policies and approaches could work in the UK.
Dame Diana Johnson: Looking at whether drugs policy reflects reality.
‘We have launched this inquiry to understand the impact of current legislation and government policy in addressing the negative consequences of drug taking in the UK,’ said committee chair Dame Diana Johnson. ‘It will look at whether drugs policy reflects the reality of drug use in the 21st century and its impact on wider society. First and foremost we want to see how well we are supporting those who are struggling with drug addiction and understand what more can be done to support them. We also want to see if efforts to combat the trade in illegal drugs have been successful and look at what has worked well in other countries.’
Meanwhile analysis from the Office for National Statistics (ONS) shows that more than 30 per cent of homicide victims over the last three years were thought to be under the influence of alcohol or illicit drugs at the time – 18 per cent had been drinking alcohol, 6 per cent had taken an illicit drug and 8 per cent were under the influence of both. Statistics for suspects were similar to those for victims, says ONS, with 28 per cent recorded to have been under the influence of alcohol and/or drugs. More than a quarter of suspects were ‘known to be drug dealers’, as were 15 per cent of victims.
This National Apprenticeship Week, members of Forward Trust’s Employment Services Directorate reflect on the delivery of the organisation’s Employability Practitioner Apprenticeship Standard.
The Employability Practitioner Standard (Level 4) is a programme that aims to upskill professionals working in the employability sector.
Why do we deliver the Employability Practitioner Apprenticeship Standard?
At Forward, we deliver a range of services, such as the Department for Work and Pensions, Restart and Kickstart for unemployed and young people who are not in education, employment, or training (NEET).
We also deliver information, advice and guidance (IAG) services in prisons. Forward is experienced in supporting people with employment. We’re well placed and proud to support, educate and train the next generation of Employability Advisors to help people bring about and sustain positive change in their lives through skilled and secure employment. This training programme began just as the government launched ‘Help to Work’ in response to the adverse economic impacts of the Covid-19 pandemic and has been operating throughout this challenging period for people seeking employment.
How do we deliver the apprenticeship?
We provide support and training for staff and apprentices from a range of partner organisations. We’re especially proud to support people with apprenticeships who have previously been supported by Forward and are now working in the employability industry. We deliver training through a blended model of face-to-face and virtual workshops, as well as providing masterclasses from Forward Trust experts and access to a range of bespoke online resources.
What did our apprentices find useful?
Our apprentices tell us that they enjoy the modular aspect to the programme and that this allows them to link different elements of learning together. For example, the linking of learning on professional standards with stakeholder engagement empowers participants to take the next step on their employment journeys. Apprentices working with us have gained knowledge and understanding of professional standards and what ‘great looks like’. This has been supported by apprentices taking on independent study into best practice industry standards such as those celebrated in the Employment Related Services Association’s annual awards.
Our apprentices work in the employability industry which often means supporting people and communities that experience disadvantage. Apprentices have benefited from Forward masterclasses to gain new skills, perspectives and understanding. This has included sessions on how Equalities, Diversity and Inclusion reporting can be used by employers to improve recruitment practices and support the creation of more diverse and representative workforces.
The first in a series of blogs by Phoenix Futures discussing aspects of residential treatment.
We recently launched a report looking at residential treatment in England, Making Rehab Matter, to highlight the severe problems people face when accessing residential treatment. The report makes recommendations about how we can work together to improve access.
Residential treatment is a clinically recommended treatment for people with multiple treatment needs. As a treatment, it is intensive, time-effective and cost-effective. Residential treatment provides an opportunity for people with a number of treatment needs to be comprehensively assessed, supported and treated in a single coordinated treatment episode.
And yet, access to residential treatment is a postcode lottery in England, with wide regional disparities of access. Whilst demand for drug treatment has increased over the last 10 years, the provision of residential treatment has declined by 50%. In some local authorities, there is no access to residential treatment at all. Overall just 0.8% of people in drug treatment can access residential treatment compared to 11% across Europe.
By working with people with lived experience, and many other stakeholders from across the drug and alcohol treatment sector, we highlighted how this dire situation could be improved to provide high-quality life-saving treatment to people who can best benefit from residential treatment.
What do international and national standards say about rehab?
There is comprehensive guidance covering access to, and provision of, residential treatment at International, National and local levels.
International Standards
The World Health Organisation published an updated International Standards for the Treatment of Drug Use Disorders in March 2020
There are extensive references to residential treatment within the standards. Under Principle 1, as an essential service, they state that residential treatment should be available, accessible, attractive, and appropriate.
The standards go on to describe the role of residential treatment in treatment systems saying that “residential treatment may be required based on an individualised assessment for those with more severe or complex drug use disorders or additional social problems.”
Whilst Section 4.1.5 covers “Specialised long-term or residential treatment” provision in detail. It covers a treatment description, target population, goals, models and key components from admission to completion.
How With You Community Link Workers are working with people in GP practices to improve their long-term health and wellbeing.
It has been an exciting journey for With You since we joined Scotland’s Community Link Worker programme back in 2019.
Our Community Link Workers work in GP practices providing non-medical support with personal, social, emotional and financial issues. These include low mood, anxiety and stress, social isolation, money and poverty issues, and bereavement.
This is one the core services available through GP practices in Scotland. They help reduce demand on primary care by diverting people to the right sources of support within the community, including welfare rights organisations and peer support groups.
With You has supported people with drugs, alcohol and mental health issues for over 50 years, giving us a lot of skill and experience in working with people in deprived communities and supporting people to change their health and wellbeing behaviour.
This experience allowed us to research and develop a brand new model for Community Link Workers. We started using this model when we won our first contract in Glasgow at the end of 2019. We received excellent feedback from clients, GPs and commissioners, with 100% of clients saying they felt:
listened to
treated with compassion, dignity and respect
connected with the right sorts of support
We built on our achievements in Glasgow by taking our model to new areas in Scotland including East Lothian, Renfrewshire and Argyll and Bute.
We now have 44 staff working across 73 GP practices. In 2021 we supported around 2,500 people.
A new taskforce to address student drug use has been launched by Universities UK (UUK) in partnership with Unite Students, GuildHE and Independent HE. The taskforce will make recommendations ‘firmly based on harm reduction’ and have student ‘safety and health at its heart’, it says, and will be advised by Professor Dame Carol Black alongside ACMD chair Professor Owen Bowden-Jones and recovery champion Dr Ed Day.
The taskforce will have student ‘safety and health at its heart’. Photo by Marko Milivojevic on Pixnio
The work will set out a ‘common approach’ to reducing harm and tackling supply, and produce evidence-led, sector-wide guidance in partnership with students, staff and others. The aim is to make student drug use ‘visible as a welfare and health issue’ with consequences for future employability, mental health and exploitation. The team will study current approaches and international best practice in support, education and treatment, as well as looking at policing and improving understanding of supply, demand and patterns of use.
Head of the taskforce, Prof Nic Beech
The taskforce, which is chaired by vice chancellor of Middlesex University London, Professor Nic Beech, will bring together sector agencies and the NUS alongside charities, government departments, accommodation providers and others, with a research report based on a wide-ranging student survey to be published later this year.
‘One of the key findings of my independent review was the rise in recreational drug use and associated harms among young adults,’ said Professor Dame Black. ‘The government’s ten-year drug strategy responded to this finding with a commitment to reducing drug use among young people. I am pleased to support this university sector-led initiative and particularly welcome the emphasis on better understanding student drug use and what works to address it.’
Over nine days in November 2021 we celebrated the harm reduction movement across the themes of science, justice and pleasure. Constellations Online Festival of Drugs and Harm Reduction, hosted by Harm Reduction International, offered a new way to connect on the big issues with the big thinkers around the world, with 1,000 participants from more than 73 countries.
DDN was proud to be a media partner and host some sessions at the event. Below you can read reports from these as well as other sessions that we were able to cover.
DDN SESSIONS
United Front: Tightening purse strings mean that the sector needs to be careful to not drift back to the bad old days of the harm reduction vs recovery wars. Jump to article
Staying Alive: Naloxone Action!, chaired by DDN, explored the vital – and often unpaid – work peers were doing to get naloxone into the hands of people who need it. Jump to article
Body positive: Peers are a group leading the fight against hep C.Jump to article
The Right Dose: An interactive session from Dr Prun Bijral and Peter Yarwood on the vital importance of making sure people were on the dose that suited them. Jump to article
OTHER DDN COVERAGE
On Message: Chemsex can be risky, but how do we get harm reduction messages to people who are young, ‘invincible’ and having fun? DDN reports. Jump to article
Stand up and be counted: Drug users have a civic duty to ‘come out of the closet’ in order to bring about real political change, Professor Carl Hart told Constellations.Jump to article
The Pleasure Principle: The ‘Last night a DJ saved my life’ session at Constellations heard from speakers across four different continents on the subject of drugs and pleasure on the dancefloor.Jump to article
Tightening purse strings mean that the sector needs to be careful to not drift back to the bad old days of the harm reduction vs recovery wars, hears DDN.
‘I’m an unapologetic and passionate harm reductionist, but I also love recovery,’ said Vicki Beere, chief executive of Project Six. ‘Both are extraordinarily important.’ She was addressing DDN’s ‘More to join us than divide us’ session at the HRI online event Constellations. However, she continued, government policy of ‘get them in, keep them in, get them out, keep them out’ when it came to services – coupled with ever-reducing budgets – was a major challenge in terms of meaningfully bringing the two together. ‘We have a really badly damaged ecosystem in drug and alcohol services. We’ve lost those small, community-rooted, passionate organisations – we’ve got a system that focuses on hitting the target but missing the point. There is hope, but we need to support each other to get there.’
Visible Recovery
Visible recovery needed to be a central element of harm reduction services, said Stuart Green, manager of Aspire Drug and Alcohol Service and a member of CLERO – ‘harm reduction and recovery is a spectrum.’ LEROs could play a vital role as they were strength-based and asset-based and recognised that individuals were the experts about themselves, he said. ‘Recovery is a very personalised experience.’
FAVOR UK CEO Annemarie Ward
It had been difficult for many in both the harm reduction field and recovery community to separate the recovery movement from the political agenda, said FAVOR UK CEO Annemarie Ward. This ‘political ramping up of language’, along with shrinking budgets and their effect on commissioning, had helped start a shift back to entrenched positions over the last couple of years, with even the word ‘recovery’ becoming tainted in many people’s eyes through its association in some areas with disinvestment. ‘It’s very human to become tribal or fixed to one particular philosophy. But the great thing about both harm reduction and recovery is that they have tremendous principles that everybody could align under if they can see the similarities rather than the differences.’
Vicki Beere, chief executive of Project Six
‘The analogy for me is that if you break your leg you want a doctor mend it but you want someone who’s previously had a broken leg to help you with recovery,’ said Green. ‘There’s a role to play for both,’ and the best intervention was always people with lived experience. ‘With person-centred services and LEROS there’s a different passion there – it’s 24/7, they don’t stop at the weekend. Meaningful change isn’t going to happen once a fortnight in a one-hour key-working session. We might be able to nudge someone, but realistically it’s about what happens in between.’ The beauty of the LERO space was that it became bigger with every person in recovery, he added.
Choices and options
People needed choices and options, said Beere. ‘There’s absolutely a real need to bring back small and medium-sized organisations – and LEROS are brilliant – that can create that flourishing ecosystem’, and commissioners needed to genuinely understand the importance of social value and localism, ‘not just a tick-box on a tender where everybody writes the same thing’. It now took genuine bravery for smaller organisations to challenge the hand that feeds, and the system needed to take account of that, she said.
Stuart Green, manager of Aspire Drug and Alcohol Service
There were some encouraging signs in commissioning however, said Green. ‘We’re seeing a bit of a paradigm shift. In terms of price versus quality, quality is creeping up more as a percentage of tenders, which is really good news, and we’re seeing longer tenders going out.’
Failure to recognise individual differences – and treatment programmes being too generic – was a major problem, said Ward. ‘It’s not just that there’s a lack of evaluation of all the recovery paths, but a lack of monitoring and real-world data around what is it that helps us get and stay well. Our job as professionals is to make sure that people have access to all the paths that will help them, and not to punish people for one particular path not working for them.’
Lived experience
‘It’s really important that we have that lived experience voice, but what we’re not very good at in our sector is getting the voice of the people who don’t access our services, who don’t get through the door,’ said Beere. ‘They’re the ones I really want to hear from. I think we’ve got a job in our sector to find and listen to that voice, even if it’s really hard to hear.’
This was especially the case in Scotland, Ward stated. ‘Sixty per cent of the people who should be in treatment are missing – they’re not even showing up. It’s not because they’re “hard to reach”. That’s usually the rhetoric, but it’s because services aren’t attractive enough.’
There were people in LEROs who had ‘never touched service land’, said Green, ‘because people do naturally recover.’ LEROs were not for everyone, he acknowledged. ‘But if you look at why people aren’t engaging in services, it’s because we’re offering the wrong thing.’
The Constellations session Staying Alive: Naloxone Action!, chaired by DDN, explored the vital – and often unpaid – work peers were doing to get naloxone into the hands of people who need it.
George Charlton (photo by Nigel Brunsden)
‘We’ve created an underclass’, said George Charlton, who works across the UK developing peer-to-peer naloxone training and supply programmes. Media headlines about ‘junkies’ had caused a disconnect between ‘some of the most socially excluded and disenfranchised people in our communities’ and the general public, he said. ‘People who do care for drug users are other users, which is why peer-led projects are so important.’
Drug-related deaths were ‘needless and avoidable’, he stated, and the most important people he worked with were those with ‘lived and living experience of addiction’. Naloxone provided a ‘wonderful opportunity to keep people alive. It’s not the whole solution, but it’s part of the solution.’
Privileged access
One of the key strengths of peer-to-peer naloxone programmes was that people who use drugs have privileged access to drug-using venues, supply systems and markets, he said – ‘they have instant trust and credibility.’ However it was vital to ensure that all organisations involved in a project were ‘fit for purpose’, he stressed. ‘We won’t recruit any peers until we’ve made sure that we’ve addressed any of the bureaucracy that could get in the way’, with everyone needing to be fully aware that lived experience often meant active drug use. ‘These aren’t recovery projects, they’re harm reduction projects.’
Community mobilisation involved asking people to ‘own and be part of’ the projects, which often meant building trust as many had been let down in the past. ‘As providers, we have the assets, the naloxone, the governance, the frameworks for peers to work within – the rooms, the teas, the coffees, the expenses. Let’s give them access to all of that, and let’s give them the project. Let’s see what the peers are doing with our support, not what “our” project is doing.’
‘The best way to get this out into the community is for drug users to go into the community,’ agreed Nottingham-based harm reduction activist and longtime DDN associate, Lee Collingham. ‘Unfortunately, the other side of my work is seeing drug users being exploited and not being paid for the work they do.’
Lee Collingham
‘We firmly believe that we cannot continue with this process of only having peers on a voluntary basis,’ stated Kirsten Horsburgh, who leads SDF’s work on drug-death prevention and is coordinator of Scotland’s national naloxone programme. ‘We absolutely need to drive home the importance of paying peers for the work they’re doing – it’s utterly crucial.’ Criminal record checks could be an unnecessary barrier for many of those eligible for doing the work, however, and while services were often able to work around this it still needed to be urgently addressed.
Scotland’s drug death situation had been described as a ‘public health emergency’ for many years without the major action to address that, she continued. ‘And then something like COVID comes along and you see how quickly things are put in place when a public health emergency is taken seriously – immediate access to resources, changes to practice, fast-tracked law changes, all the things we really require for addressing the drugs death crisis.’
Progressive
Kirsten Horsburgh
The country’s naloxone programme had been in place since 2011, however, supplying more than 100,000 take-home kits. ‘Scotland has been fairly progressive in a number of areas around distribution,’ she said, despite legal restrictions, and with a national awareness campaign in place since August (DDN, September, page 4). ‘The focus for the campaign we were commissioned by the Scottish Government to deliver is about a wider societal response,’ not just targeting people who use drugs or their families – ‘every single person can do something.’ More than 30,000 people had visited the Stop The Deaths website in ten weeks, with much of the feedback – especially from family members and people who use drugs themselves – emphasising that ‘just seeing that on such a public platform, on mainstream TV and across the country, was really powerful – that recognition that these lives matter.’
In the first year of Nottingham’s naloxone programme ‘we spent less than £2,000 and over 100 overdoses were reversed’, said Collingham. ‘That’s 100 families that still had loved ones.’ As one of the faces of the national naloxone billboard campaign (DDN, May, page 12), he was able to choose his own message to go alongside his image. ‘As someone who’s carried both it was clear to me that carrying naloxone is easier than carrying a mate’s coffin. Let’s have our loved ones at home, and let’s carry naloxone.’
Peers are a group leading the fight against hep C, hears DDN.
‘I love what I do,’ Paul Huggett, peer coordinator for the Hepatitis C Trust, told the Positive about being positive session at HRI’s Constellations harm reduction festival. ‘When I give someone the diagnosis that they’re positive but then tell them I’ve had it, they say, “but you look well”. I say, “exactly”.’
Paul Huggett
There had been a significant year-on-year increase in the number of people being treated since 2017, said Hepatitis C Trust regional manager, Danny Morris, but there was still a long way to go when it came to reducing chronic infections, particularly in the wake of COVID-19. Rates of equipment sharing, meanwhile, were still around 25 per cent – ‘a big, big concern for us’ – and around half of those living with hepatitis C were still unaware of their status. The trust delivered peer projects across the UK, he said, working closely with hepatology teams, drug and alcohol services, homelessness services and prisons, with the majority of staff having lived experience. One vital aspect of their work was modifying and speeding up pathways into treatment, particularly for more marginalised communities.
Individual need
‘That’s a big part of it,’ said Nathan Motherwell, a peer coordinator for the trust. ‘For example, they don’t write to homeless people at the drug service anymore.’ He helped to make sure that treatment was adapted to suit people’s individual needs and coordinated and recruited other peers, using his experiences to build rapport with his clients. ‘I was a very chaotic drug and alcohol user, but all of the things I experienced – even including prison – have ended up being useful in some way. When I talk to people I say, “I used to do that”, and it breaks down some of that shame.’
Nathan Motherwell
Elimination was now becoming a reality, partly through treating whole communities of injecting drug users in different locations – ‘we’ve probably significantly reduced the risk of anyone getting hep C in the Medway towns over the last three years.’ The key was to ‘be persistent and don’t take it personally,’ he said. ‘Sometimes people don’t want to engage. I’ve been sworn at when people are busy trying to score, I’ve booked people several appointments and two years later they eventually say they’re ready to do it. They’ll come round in the end.’ There was often an intense level of support needed, particularly for clients with dual diagnosis, and this involved working closely with other agencies. ‘These are the people with the highest risk of reinfecting themselves or infecting others. But we’ve got good outreach teams and they know these people.’
People often lied, he said, partly because of the shame. ‘But if you break down the practice – who they use with, when, where and how, you can often change one little bit and that might help.’ This could be something as simple as getting people to carry their own equipment, spoon or bottle of water. ‘Some of the peers are still on methadone scripts so they’re a lot closer to where people are at, and have managed to engage people that I couldn’t.’ Clients were also encouraged to find other people for testing in exchange for vouchers, he said – ‘sometimes people will turn up with five others.’
Education and prevention
Education and prevention were vital, said Huggett, who was in active addiction for 20 years. ‘We all know it’s full of fear and stigma, but if you start talking about it, it eases all that stuff.’ Having a regular presence at hostels and drop-in centres for testing days was also crucial, he said. ‘If they keep seeing us, eventually they’ll get tested.’ It was about ‘being consistent with love, care and compassion – they’re going to come round and we’re going to get them.’
He coordinated a team of four peers with eight volunteers, and a current project involved target-testing in a pharmacy. ‘The more testing you do, like with COVID, the more positives you find.’ But it was then vital to make sure the right level of support and care was in place to get them through treatment. ‘Gold standard is not knowing they’re positive and leaving them out there.
The Best job
‘It’s about more than hep C,’ he stated. ‘Once they told me I’d got the all-clear it made the impossible possible. It made getting stable on a script seem doable, even sobriety seemed achievable. Because I’d just beaten a killer disease. I’ve got the best job in the world because every week I’m telling people they’ve got the all-clear from hep C.’
The DDN-hosted The Right Dose session at Constellations heard from Dr Prun Bijral and Peter Yarwood on the vital importance of making sure people were on the dose that suited them.
‘Everyone’s individual needs are individual – and unique,’ said Dr Prun Bijral, medical director at Change Grow Live. ‘It’s about the balance of getting that dose right for them. In a nutshell, we’re trying to help people stay comfortable and get some stability in their lives.’
Peter Yarwood
People entering treatment services were often at a very low point, so it was vital to build relationships that were based on trust and honesty in a supportive environment, said Peter Yarwood, founder of Red Rose Recovery and in long-term recovery himself. ‘You’ve got people at different stages, who might not know what’s right for them – that’s got to be a process, it can’t be fixed in one visit.’
Treatment quality
Ultimately, whether people felt they were able to speak honestly came down the quality of the treatment, Bijral told the session. ‘As a doctor I’m not going to be able to do my job if I don’t know what the real issue is. What I will always say to people is, “it’s your treatment”. It’s for us to serve and make that treatment as accessible, practical and useful as possible.’ Clinicians had to recognise that entering treatment was very often a ‘make or break’ situation for people, and it was vital that they did everything they could to make them feel comfortable and informed. ‘You have to be there for them, rather than have some agenda of “I’m going to get you on this or that”.’
It all came down to the quality of the relationship, added Yarwood. ‘Everybody wants to help people improve their wellbeing and get to their destination, but that’s not to say we might not get it wrong. But if we do we need to be mature enough to open up a space to explore that without taking it as a personal criticism.’
Bringing about culture change across the sector and addressing sub-optimal treatment depended on education, said Bijral. ‘Demystifying treatment – it’s not rocket science. Get the dose that helps that person feel comfortable.’ Change Grow Live had made the guidance more accessible to its frontline staff, modified its training and, crucially, showed services what their treatment looked like. ‘Those same issues persisted, people were underdosed, were using when they didn’t want to – we weren’t providing the treatment for the need, it was as simple as that. But when you start showing people that, they automatically start to change and have different conversations.’
Stigma remained a significant issue, however. ‘The solution is broader than a clinical one, it’s a social one,’ said Yarwood. ‘There’s work that needs to be done to educate the community, and then highlight the support available.’ People were now able to put their own stories out on other platforms without needing to go via news outlets, however – ‘we can counterbalance the negative voices.’
Opportunity for Change
The Carol Black report was a crucial opportunity for change when it came to the central role of peers – ‘it’s not about hearing that voice, it’s about enabling people to take control of things like commissioning, of policy,’ said Bijral. This had been one of the few silver linings of the pandemic, he added. ‘We can’t just go, “Yeah, we’re hearing you” now’ – the people most affected by the system and change needed to be the ones shaping it. ‘Then you’re going to have a better system and a better service. It’s not going to be easy, it’s complex – without question – but you’ve got to start at the principles.’
Dr Prun Bijral
Postcode lotteries remained a recurrent issue, but providers had to make sure their practice was in line with the evidence-based guidance, stressed Bijral. ‘That’s key – not just, “I fancy providing this dose because that’s how I woke up this morning.” Our services aren’t about fancy machines, they’re about people, so you’re going to get differences. But it comes down to awareness and shining a light on the treatment that’s being provided. We’ve got to move more towards a focus on quality and what people deserve, and view it from people’s perspective – not a provider perspective, or a commissioner perspective. It’s got to be about the person.’
Drug users have a civic duty to ‘come out of the closet’ in order to bring about real political change, Professor Carl Hart told Constellations.
Professor Carl Hart
‘Drug control has been used as a tool to subjugate, and has its origins in subjugating specific populations – certainly in the US,’ Professor Carl Hart of Columbia University told Harm Reduction International executive director Naomi Burke-Shyne. ‘That’s why it’s important to question the basic assumptions of drug control.’
One of these was that the government ‘does not trust you to make the right decisions about what you can put in your body’, he said, something that was then backed up with vast amounts of money. ‘When you think about all the people who are employed in order to control what you put in your body’ – not just law enforcement and prison authorities, but researchers, physicians, the media – ‘all of these people have their hand in the cookie jar. That’s the real reason this continues, and it helps that the people who are primarily impacted are poor and politically weak.’
Assertions that the ‘war on drugs’ had somehow failed were therefore wrong. ‘It’s been a success for the people in control, and the people they give their fruits to’ – the ‘war on drugs’ was essentially a jobs programme, he said. ‘If we think that the stated policy is to lessen the availability of these substances in our communities, then at some level it did that. But the unstated goal is to increase the budgets of various groups of people, and it worked there as well.’
One useful aspect of cannabis reform in the US, therefore, was demonstrating to the ‘people who have power in our society how they can make money off this endeavour – legally regulating the market,’ he said. ‘We’ve seen how the human rights violations, racial discrimination and targeting of poor people hasn’t been compelling at all. So we need to really think about how we advocate for change.’ There was also a huge amount of people ‘who – although we might not agree on a number of political issues – really understand the concept of liberty’, he stated. ‘At this basic fundamental level of people’s liberty, we agree.’
If governments saw drug users as people with political power and a vote ‘then maybe we wouldn’t have so many repressive laws that have targeted people with less political power’, he said, which was why he tried to encourage people to ‘get out of the closet’ about their drug use as a matter of civic duty. The majority of people using drugs were simply ‘seeking to alter their consciousness,’ he continued, so ‘why aren’t we defending their liberty to take them? The vast majority of users of any drug don’t meet the criteria for addiction.’
On the question of worrying about who would ultimately control the regulated market, there were more pressing concerns, he told the session. ‘We’ve yet to even have a serious conversation about legally regulating the market. The first goal is to take the chains off, then we can worry about who’s controlling it.’
There had always been a disproportionate focus on the negative aspects of drug use and it was time to talk about the positive aspects, such as pleasure, he added. ‘I upset so many people by saying that sort of thing. Pleasure is a good thing, and it’s sad that I even have to say that.’
On the question of changing the language around drug use, while it was as important to be precise ‘we don’t want to get hung up too much on it’, he said. ‘Stay focused on the big issue, which is do people have the right to put whatever drug they want in their bodies. There’s always risk when you’re fighting injustice, but it causes a lot more harm not to do anything.’
The ‘Last night a DJ saved my life’ session at Constellations heard from speakers across four different continents on the subject of drugs and pleasure on the dancefloor.
Dr Giulia Zampini
‘I’m a clubber, and I didn’t feel the experience of clubbing was particularly well-represented in mainstream narratives and discourses,’ senior lecturer in criminology at the University of Greenwich, Dr Giulia Zampini, told the Last night a DJ saved my life: a meaningful discussion on the role of drugs and pleasure on the dancefloor session. ‘There was a lot of stigma and misunderstanding.’
She had launched a project called ‘People and dancefloors’ in order to bring clubbing stories to life, emphasising the positives – including taking drugs. ‘It was quite refreshing to see how people were more than willing to share, coming out about their drug use on camera, which in many contexts – including the UK – can have repercussions in terms of reputations and jobs.’
‘I’ve always been an avid partygoer,’ Ayodeji Ayoola, a Lagos-based cinematographer, told the session. ‘But drug use in Nigeria is generally illegal, including alcohol in some parts of the country where you could get arrested for drinking a bottle of beer.’ There was almost no positive conversation about drug use in his country, he said – ‘and zero conversation about pleasure. It’s sad, but it is what it is.’
‘I share with many drug users and women the pressures of guilt in many everyday situations – the personal is political,’ said Columbia-based Alejandra Medina of the Acción Técnica Social NGO. Her organisation worked closely with partygoers, party organisers and the media on issues of harm reduction and pleasure enhancement, and to get across the message that ‘substance users can actually enjoy themselves without guilt and without risk. As the others mentioned, raving and having fun is stigmatised and seen as immoral, even in the 21st century’. Her organisation was often condemned for being ‘promoters’ of drug use, she said.
Not being honest about the benefits and pleasures of drug use had been a ‘real disservice’ to the harm reduction movement, said Mitchell Gomez, executive director of US-based organisation DanceSafe. ‘People are so heavily propagandised by the drug war, and taught things that are just demonstrably untrue. Even the term “harm reduction” implies that harms are intrinsic to drug use. It’s deeply concerning to me that we focus so heavily on the harms when the vast majority of people are non-problematic substance users – they’re just people who use drugs.’
Many of his organisation’s activities, such as drug checking, were less harm reduction than ‘drug prohibition harm reduction’, he said. ‘If there were legal, regulated markets, then most of what DanceSafe does wouldn’t be necessary. The existing UN declaration on Human Rights is entirely incompatible with governments telling you what substances you can or cannot use – the drug war is fundamentally an anti-human rights policy. As harm reductionists and public health professionals we need to start being very, very honest about the fact that most users benefit and receive pleasure from their drug use.’
‘We need to come out of the psychoactive closet,’ agreed Medina. ‘We want to empower our collective right to have a pleasurable experience, and we need to be able to shake off that guilt that’s more about the lack of market regulations and the political will to accept that a drug-free world is not possible.’
While the dancefloor was one place where pleasure-seeking was more allowed than in others, in wider society there remained a ‘double social taboo’, said Zampini, with both drugs and pleasure itself in many ways still taboo subjects. ‘We keep pleasure as a dirty secret,’ she said, partly because of a religious underpinning that pleasure was sinful and something to be controlled or repressed.
Although manifested differently, this was shared across all cultures, she said. ‘We still carry the remnants of that – this is where we’re still at. But we’re all driven by pleasure, we’re all pleasure-seeking beings.’
People’s perceptions of drugs had been framed by prohibition, but it was fair to say that many pleasurable activities, including sports, carried some risk, she continued, and one way to move away from concepts of guilty and risky pleasures was to foreground mental health. ‘People are passionate about it, and it gives individuals the power to advocate for their own health. So they can say, “My experience of taking ecstasy is that it makes me feel good’. I feel we should really harness that shift to transform the discussion. Maybe then we can start talking about healthy pleasures.’
‘As the years go by there will be change,’ said Ayoola. ‘Whether it’s slow or fast it’s change, and we’ll take whatever it is we get.’
Chemsex can be risky, but how do we get harm reduction messages to people who are young, ‘invincible’ and having fun? DDN reports.
Patriic Gayle, The Gay Men’s Health Collective
‘A lot of harm reduction information is coming through specialist services, and you have to be quite far down the road before you pitch up at a specialist service,’ – something that applied equally to hepatitis C, drug use or chemsex, said Leila Reid of the Hepatitis C Trust. ‘So how do you reach people at the beginning so that they know to look for harm reduction information?’
People who were ‘younger and feeling invincible and having fun’ wouldn’t necessarily want to hear these messages, said Patriic Gayle of the Gay Men’s Health Collective. Many of the victims of serial killer Stephen Port, however, who used GHB on his victims (DDN, February 2020, page 4) were so unaware when it came to drugs issues that they could ‘be lured into a situation where they could be given fatal overdoses’, said Bob Hodgson, independent advisor with the Metropolitan Police Service.
Service integration
A key point was integration of services, said Reid, not just with drugs and sexual health but across the board, and there had been excellent work in London and elsewhere around integrating HIV and hepatitis C testing and using those chances to deliver harm reduction information. ‘There’s a lot of opportunity when you’ve got that person there. For hep C at the moment there’s a bit more of a focus and energy around it, so maybe we’re reaching people who aren’t normally reachable by health systems. From a general public health perspective, there’s this idea of making every contact count, which is quite well established in some parts of health and social care as well as housing – there are a lot of agencies that come into contact with people at different, difficult times.’
Vital Resources
The Gay Men’s Health Collective had been running a pilot project of making their chemsex resources available in A&E, said Gayle. ‘We know that in one A&E you’re looking at between five and ten admissions on a weekly basis for GHB overdose, and in terms of what they’re rather disparagingly calling “frequent flyers”, they’ll quite often have return visits.’
The material was an accessible, cost-effective tool, and the plan was to roll the programme out further, he said. ‘What we discovered was that staff were saying they could finally give people something to take away with them.’ Healthcare workers often didn’t feel confident discussing certain issues with patients, said Reid – ‘something like this can really open up a discussion in a much easier way’.
Information detailing people’s rights on arrest was also important, said Hodgson, especially when someone overdoses. ‘If someone’s read a “bust booklet” when they’re not already taking drugs and are able to absorb the information then that’s there when they’re thinking “should I or shouldn’t I call an ambulance?” So they know they’re not just subject to the whim of whatever policeman turns up at the door, they have rights and there are protocols and people they can contact. When the paramedics get there you do need to take a leap of faith – you need to tell them what they’ve taken so they can treat them properly – but, with good will and sensible policing and ambulance services, they’ll concentrate on the health needs and not bother about the drug.’
As Dame Carol Black’s report pointed out, sizeable gaps remained around harm reduction when it came to communities who didn’t really identify with the injecting population, said Reid, ‘particularly MSM involved in chemsex, people using steroids and performance-enhancing drugs.’
‘Harm reduction, public health, wellbeing messaging around safer drug use and chemsex would be helpful in terms of hopefully reducing the number of people who end up being admitted to hospital,’ said Gayle. ‘We don’t have that, and it worries me that in the present climate it’s struggling to get traction. I understand why, but if we don’t do something about it we have a perfect storm.’
‘You’re reducing the stress on the police force, the ambulance services,’ said Hodgson. ‘It’s a small amount of money that should save a lot down the line.’
Prevention
Prevention was always vastly more cost-effective than treatment, agreed Reid, but less easy to make the business case for, ‘particularly if it’s a population that a lot of people don’t have a great deal of sympathy for. But if you can engage people you can address mental health and whatever else is there – early intervention and being proactive means you can prevent hep C, HIV and overdose and work really constructively with people. That’s what’s important if we want to really change people’s outcomes on a big scale.’
It’s National Apprenticeship Week 2022 and Forward is celebrating the great work of apprentices, their employers and the families and networks that support them.
With the economy beginning to bounce back, it has been good to see the number of people starting apprenticeships in England higher in 2022 than in 2021, up 43% from the same period in last year.
As a growing Information, Advice and Guidance (IAG), Adult Education Budget, employability and apprenticeships provider, at Forward we can see how apprenticeships help individuals to develop their skills, knowledge and behaviours to support them towards a rewarding career.
Apprenticeships can improve social mobility
According to the Social Mobility Commission, ‘apprenticeships are one of the few indisputably effective tools of social mobility currently available to the government. There is evidence to confirm the benefits they confer on workplace learners – such as enhanced career earnings, continued education and richer, more fulfilled working lives.’
We are proud that 40% of the apprentices we support as a Real Living Wage employer through the Forward Trust levy have experience of being in recovery, the criminal justice system or unemployment. We support training that allows apprentices to enjoy the benefits of learning whilst earning in addition to a range of other positive advantages. For example, apprentices improve their social capital (building their personal connections and networks), enhance their cultural capital (building confidence in workplace communication) and demonstrate a high level of confidence and aspirations for the future.
However, the Social Mobility Commission identifies gaps for people from disadvantaged backgrounds in employer recruitment and selection for apprenticeship training; the quality or ‘value’ of the training received; the likelihood of completing training and of progressing into higher-level apprenticeships, or high paid jobs.
That is why this National Apprenticeship Week we are urging employers and providers to give amazing learners from all communities and experiences a chance as an apprentice and to offer them the support and guidance they need to succeed and progress from their apprenticeships into rewarding careers.

 As far back as 2002, research was showing that 70 per cent of people in drug services and 86 per cent in alcohol services had described or reported severe mental health problems in the previous year, said Dr Hauwa Onifade, a forensic psychologist at Turning Point involved in developing services with an integrated approach to co-existing mental health difficulties and substance use. Far too many in this client group were still failing to access the support they needed, she said.
As far back as 2002, research was showing that 70 per cent of people in drug services and 86 per cent in alcohol services had described or reported severe mental health problems in the previous year, said Dr Hauwa Onifade, a forensic psychologist at Turning Point involved in developing services with an integrated approach to co-existing mental health difficulties and substance use. Far too many in this client group were still failing to access the support they needed, she said. Turning Point had developed a substance use and mental health (SUMH) toolkit for professionals, condensing research and guidelines from PHE, NICE and elsewhere, she said. The organisation had also been working in Leicester, Leicestershire and Rutland on developing an integrated team, with a pilot launching during the COVID period following an audit of more than 3,000 clients. This had identified two significant groups where there were gaps in accessing treatment – populations involved in injecting drug use who were ‘frequent flyers’ at local hospitals and also presented with high levels of risk around mental health, including self-harm and suicide, and longer-term clients who, although there was little risk of self-harm or suicide, were in high levels of distress and unable to make changes in their substance use as a result.
Turning Point had developed a substance use and mental health (SUMH) toolkit for professionals, condensing research and guidelines from PHE, NICE and elsewhere, she said. The organisation had also been working in Leicester, Leicestershire and Rutland on developing an integrated team, with a pilot launching during the COVID period following an audit of more than 3,000 clients. This had identified two significant groups where there were gaps in accessing treatment – populations involved in injecting drug use who were ‘frequent flyers’ at local hospitals and also presented with high levels of risk around mental health, including self-harm and suicide, and longer-term clients who, although there was little risk of self-harm or suicide, were in high levels of distress and unable to make changes in their substance use as a result.
 Oasis’ approach includes delivery of treatment in a women-only building, providing a physically and emotionally safe place for women to access support in an environment which recognises the prevalence of trauma and actively seeks to prevent re-traumatisation and promote recovery. Women report feeling more comfortable in a setting they know is women-only, sharing space with peers and drawing on shared connections, without risk of being in groups and settings with a partner, or ex-partner.
Oasis’ approach includes delivery of treatment in a women-only building, providing a physically and emotionally safe place for women to access support in an environment which recognises the prevalence of trauma and actively seeks to prevent re-traumatisation and promote recovery. Women report feeling more comfortable in a setting they know is women-only, sharing space with peers and drawing on shared connections, without risk of being in groups and settings with a partner, or ex-partner. Case studies
Case studies Taking Control
Taking Control



 Release are UK experts on drugs and drug laws and provide advice and advocacy. A non-government and non-profit organisation, they campaign for drug policies that respect
Release are UK experts on drugs and drug laws and provide advice and advocacy. A non-government and non-profit organisation, they campaign for drug policies that respect

 We are proud to work in partnership with many of the leading charities and treatment providers in the sector.
We are proud to work in partnership with many of the leading charities and treatment providers in the sector.



 While all local authorities will receive additional funding as part of the government’s three-year £780m investment in treatment
While all local authorities will receive additional funding as part of the government’s three-year £780m investment in treatment 





 My work background before I went to prison was mainly machine driving, but also building and construction, warehouse jobs and driving jobs. I’ve had spells off from time to time due to factors going on in my life, whether it be drink, drugs, family issues, poor emotional management, or not being able to cope properly. But I’ve always worked, and I’ve always managed to get myself a job and have a bit of stability.
My work background before I went to prison was mainly machine driving, but also building and construction, warehouse jobs and driving jobs. I’ve had spells off from time to time due to factors going on in my life, whether it be drink, drugs, family issues, poor emotional management, or not being able to cope properly. But I’ve always worked, and I’ve always managed to get myself a job and have a bit of stability. By 2000, I was completely out of control, barely hanging on to my job, and I went to the first of six treatment centres. When I left, I should have gone to a ‘dry house’, but I chose not to – I wanted to return to work. I returned to work five weeks after leaving and relapsed within a week. By 2001, my employer said, ‘We need to part company with you’.
By 2000, I was completely out of control, barely hanging on to my job, and I went to the first of six treatment centres. When I left, I should have gone to a ‘dry house’, but I chose not to – I wanted to return to work. I returned to work five weeks after leaving and relapsed within a week. By 2001, my employer said, ‘We need to part company with you’.

 The team brandish naloxone kits when they’re out and about – a conversation starter as well as a vital harm reduction intervention. They wear their naloxone shirts and are proud to spread the word as Medway naloxone peers. On their route down the high street they stop to talk to two young men who are willing to hear more and engage in answering some questions – ‘What are the main causes of an overdose? When are the high-risk times? What are the signs and symptoms of an overdose? What should you not do in an overdose situation…?’ The men carry on their way with naloxone kits and the knowledge and confidence to use them, saying they ‘learned something very useful’.
The team brandish naloxone kits when they’re out and about – a conversation starter as well as a vital harm reduction intervention. They wear their naloxone shirts and are proud to spread the word as Medway naloxone peers. On their route down the high street they stop to talk to two young men who are willing to hear more and engage in answering some questions – ‘What are the main causes of an overdose? When are the high-risk times? What are the signs and symptoms of an overdose? What should you not do in an overdose situation…?’ The men carry on their way with naloxone kits and the knowledge and confidence to use them, saying they ‘learned something very useful’. As they work through an agenda that covers their progress over the last few months they realise their partnership working is paying off and results are tangible – for clients and for the team members themselves. The growth and development of the peer group is an important part of this story.
As they work through an agenda that covers their progress over the last few months they realise their partnership working is paying off and results are tangible – for clients and for the team members themselves. The growth and development of the peer group is an important part of this story.
 Jo Payne, volunteer and building recovery coordinator, has worked with Open Road since 2018 and has seen the peer support develop as the partnerships have evolved. The peer projects now reach into all areas of work – outreach, naloxone, sexual health, the hep C clinic, rough sleeper initiatives with the council, the Ladies’ Night project with sex workers. With 24 peer mentors, ‘it’s known as a safe place to be,’ she says. Furthermore, ‘peer mentor support has become integral to services’ and peer mentors regularly work at Turning Point, co-facilitating groups.
Jo Payne, volunteer and building recovery coordinator, has worked with Open Road since 2018 and has seen the peer support develop as the partnerships have evolved. The peer projects now reach into all areas of work – outreach, naloxone, sexual health, the hep C clinic, rough sleeper initiatives with the council, the Ladies’ Night project with sex workers. With 24 peer mentors, ‘it’s known as a safe place to be,’ she says. Furthermore, ‘peer mentor support has become integral to services’ and peer mentors regularly work at Turning Point, co-facilitating groups.
 Gambling and lottery advertising will no longer be able to use content ‘likely to be of strong appeal to children or young persons’, the Committee for Advertising Practice (CAP) has announced, especially that associated with youth culture. This means that prominent sports personalities, celebrities and social media influencers will no longer be able promote gambling brands if they strongly appeal to those under 18.
Gambling and lottery advertising will no longer be able to use content ‘likely to be of strong appeal to children or young persons’, the Committee for Advertising Practice (CAP) has announced, especially that associated with youth culture. This means that prominent sports personalities, celebrities and social media influencers will no longer be able promote gambling brands if they strongly appeal to those under 18.


 A letter from a prisoner had pointed out that any attempt to tackle alcohol and drug-related deaths in custody would need to address ‘many aspects’ of prison life. ‘It’s the overall context in which people are living, and of course this has been exacerbated massively by COVID. The kind of desperation we’ve been seeing, the crushing boredom, living 23 hours a day in a six-by-nine cell often shared with a stranger.’ It was clear why people would turn to ‘any substance’ to try to block this out, she said. Unless someone had gone through it they could ‘never comprehend’ it, the letter had stressed.
A letter from a prisoner had pointed out that any attempt to tackle alcohol and drug-related deaths in custody would need to address ‘many aspects’ of prison life. ‘It’s the overall context in which people are living, and of course this has been exacerbated massively by COVID. The kind of desperation we’ve been seeing, the crushing boredom, living 23 hours a day in a six-by-nine cell often shared with a stranger.’ It was clear why people would turn to ‘any substance’ to try to block this out, she said. Unless someone had gone through it they could ‘never comprehend’ it, the letter had stressed.


 Housing Matters
Housing Matters









 More than half of the people who changed from buprenorphine to Espranor remained on the same dose at the point of switching (Figure 2), and a large proportion of people remained on the dose they started Espranor on after 28 days of treatment (Figure 3). A larger proportion of people required a dose change within 28 days of starting Espranor treatment if they changed dose at the point of switching from sublingual buprenorphine, and if people needed to change dose after starting Espranor they were more likely to need a dose increase than decrease.
More than half of the people who changed from buprenorphine to Espranor remained on the same dose at the point of switching (Figure 2), and a large proportion of people remained on the dose they started Espranor on after 28 days of treatment (Figure 3). A larger proportion of people required a dose change within 28 days of starting Espranor treatment if they changed dose at the point of switching from sublingual buprenorphine, and if people needed to change dose after starting Espranor they were more likely to need a dose increase than decrease.
 An outreach worker reports that people find Espranor less intrusive when doses are being supervised, and that Espranor feels more dignified as people do not have to stand in the pharmacy for a long time waiting for the dose to dissolve. They also echo service user feedback that Espranor tastes better. Staff report reduced diversion risk as a key benefit, and they are more assured that people are taking their prescribed dose.
An outreach worker reports that people find Espranor less intrusive when doses are being supervised, and that Espranor feels more dignified as people do not have to stand in the pharmacy for a long time waiting for the dose to dissolve. They also echo service user feedback that Espranor tastes better. Staff report reduced diversion risk as a key benefit, and they are more assured that people are taking their prescribed dose. 






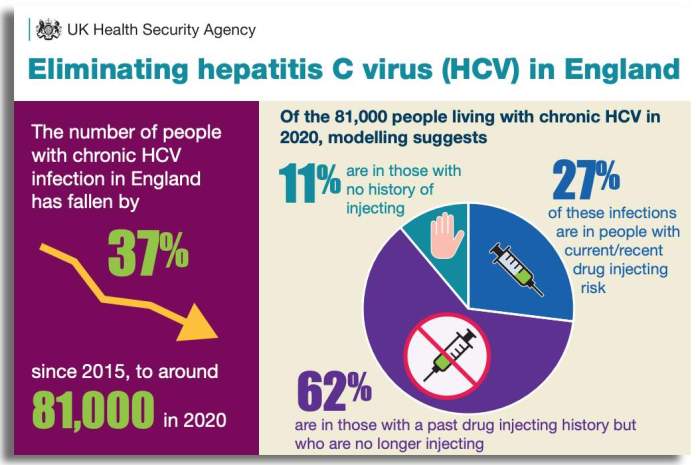












 The group, which is chaired by Humankind, has already submitted a letter to the Office for Health Improvement and Disparities (OHID) outlining the minimum provision for women that should exist in every service.
The group, which is chaired by Humankind, has already submitted a letter to the Office for Health Improvement and Disparities (OHID) outlining the minimum provision for women that should exist in every service. 




 The highest number of deaths occurred in the 35-39 age group, followed closely by the 40-44 age group. The age profile of overdose deaths followed the same pattern, but with a more pronounced peak in the 35-39 age group. The data suggests that those aged 50 and over are more likely to die from a physical health condition than an overdose – in the 50-plus age group 19 per cent of deaths were due to overdose, compared to 39 per cent of deaths in those aged 35-49.
The highest number of deaths occurred in the 35-39 age group, followed closely by the 40-44 age group. The age profile of overdose deaths followed the same pattern, but with a more pronounced peak in the 35-39 age group. The data suggests that those aged 50 and over are more likely to die from a physical health condition than an overdose – in the 50-plus age group 19 per cent of deaths were due to overdose, compared to 39 per cent of deaths in those aged 35-49. Physical health conditions were highly prevalent in the cohort that died, with 81 per cent of people (251) having at least one such condition – 60 per cent (186) had two or more. The most commonly occurring conditions were chronic obstructive pulmonary disease (COPD) at the time of death. In this study 243 decedents were under the age of 50. Of these 191 had at least one long-term health condition such as COPD, liver disease, or a heart condition, and 155 had an identifiable mental health condition, such as anxiety and depression disorders, personality disorder, PTSD or psychotic illness. Poor physical health and life-limiting conditions will continue to be a challenge to the sector. Three quarters of the people who died had also had at least one hospital admission in the previous 12 months – a significant red flag and a clear indicator of risk regardless of reason for hospital admission.
Physical health conditions were highly prevalent in the cohort that died, with 81 per cent of people (251) having at least one such condition – 60 per cent (186) had two or more. The most commonly occurring conditions were chronic obstructive pulmonary disease (COPD) at the time of death. In this study 243 decedents were under the age of 50. Of these 191 had at least one long-term health condition such as COPD, liver disease, or a heart condition, and 155 had an identifiable mental health condition, such as anxiety and depression disorders, personality disorder, PTSD or psychotic illness. Poor physical health and life-limiting conditions will continue to be a challenge to the sector. Three quarters of the people who died had also had at least one hospital admission in the previous 12 months – a significant red flag and a clear indicator of risk regardless of reason for hospital admission. A partnership between Derbyshire Healthcare NHS Foundation Trust and ImpACT+, the specialist respiratory/COPD team based at the Royal Derby Hospital, was created to address a recognised need for access to specialist respiratory care for those using our services. This service is now delivered from within two of our treatment bases. More people have been diagnosed and commenced on treatment regimes, with one case of TB identified and treated. Many with symptoms but undiagnosed have been identified and received appropriate investigations for symptoms they had previously not addressed or been unable to access their GP to discuss. One client was identified to be suffering from a range of conditions including a DVT and heart failure and is only alive today because the health improvement nurse had access to the specialist team who were able to act accordingly on her concerns.
A partnership between Derbyshire Healthcare NHS Foundation Trust and ImpACT+, the specialist respiratory/COPD team based at the Royal Derby Hospital, was created to address a recognised need for access to specialist respiratory care for those using our services. This service is now delivered from within two of our treatment bases. More people have been diagnosed and commenced on treatment regimes, with one case of TB identified and treated. Many with symptoms but undiagnosed have been identified and received appropriate investigations for symptoms they had previously not addressed or been unable to access their GP to discuss. One client was identified to be suffering from a range of conditions including a DVT and heart failure and is only alive today because the health improvement nurse had access to the specialist team who were able to act accordingly on her concerns. Engage and re-engage
Engage and re-engage




 The intimidating men-only environments of betting shops meant that problem gambling was largely a male problem, but the rise of online gambling has changed all that.
The intimidating men-only environments of betting shops meant that problem gambling was largely a male problem, but the rise of online gambling has changed all that. 










































