

Encouraged by results of a new form of community opiate detoxification, a team from substance misuse services in Bristol and the South West offer their ‘recipe for recovery’ .
The landscape for addiction treatment is changing. Since 2001, there have been three phases in the modernisation of treatment for substance misuse problems – access, retention, completion – that brought us to where we are now. We are now in an evolving fourth phase which is about producing real world recovery outcomes.
As a result of the Health and Social Care Act 2012, the public health function was transferred from the health service to the 152 local authorities. It is difficult to see where the investment in drug treatment is going with any precision but the direction is very clear; it is going down. Duncan Selbie, chief executive of Public Health England, addressed substance misuse commissioners and providers at a recent conference in Bristol entitled Sustainable recovery solutions. He highlighted the need to think and work smarter in these times of austerity: ‘The music has changed – you need to learn a new dance!’

Ironically, tightening budgets might be good news for abstinence-based community recovery. At the same conference, we noted that the current and evolving focus on real world social outcomes (such as jobs, homes, family and friends) offers great opportunities for the development of abstinence-based recovery and this reinforces a focus on innovation, improved outcomes and increased value.
As previous and current providers of substance misuse services in Bristol and the South West, we feel that our ‘detox in a box’ model demonstrates those very objectives – innovation, improved outcomes and increased value. However, not being the best of dancers, we prefer to liken it to cooking – our ‘recipe for recovery’.
Innovation
Back in 2010, South Gloucestershire Drug and Alcohol community services introduced a novel two-week community opiate detox protocol, which was created to address the problem of a long backlog of service users awaiting a structured opiate detox against a climate of limited bed availability for a medically supervised detox.
At this time, the practice was mainly focused on substitute prescribing and risk minimisation. The ‘detox in a box’ protocol brought a shift in mindset towards recovery and abstinence as well as higher aspirations for service user success, bringing hope back into the hearts of both clients and staff.
Improved outcomes
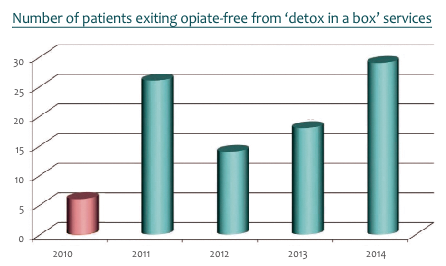
‘Detox in a box’ was rapidly embraced by both key workers and service users and proved highly successful over the subsequent four years, leading to a dramatic improvement in the number of service users exiting drug-free from our services. In the first year after its introduction, the number of patients achieving abstinence quadrupled. This dramatic improvement cleared the backlog of highly motivated clients waiting for a detox. Subsequent years showed a similar steady increase in the numbers of those achieving abstinence.
Unlike opiate detox methods involving gradual dose reduction, which may feel like an endless ‘Russian doll’ game (often ending up as long-term sub therapeutic OST prescribing), ‘detox in a box’ gave our service users a clear goal: the prospect of attaining abstinence in only 14 days. It also switched the client’s focus from the detox process, to the real and more deserving challenge of maintaining abstinence and recovery.
Increased value
Aside from the clear benefits of our clients having an improved chance of actually completing their detox, we found that running this model alongside the existing alcohol detox service made better use of resources – both in terms of facilities and staff. Having a programme that was time limited, with a clear beginning, middle and end, also enabled us to plan aftercare services more effectively. We also found that working alongside mutual aid groups such as SMART Recovery and NA was an essential ingredient in the success of the model. Using our existing relationships with our colleagues in community pharmacies helped to add another layer of support.

Who is it for?
As with cooking, a dish only suits some people but not others. ‘Detox in a box’ best suits patients stabilised on methadone or buprenorphine, highly motivated to detox in the community within a short period of time and with no major psychiatric or physical health co-morbidities. It is unlikely to be successful for those still using heroin exclusively or on top of methadone.
Challenges
Before implementing this approach, we were disheartened by the number of service users who had been held on non-therapeutic doses of methadone and buprenorphine for long periods of time, because of fear or anxiety about the opiate withdrawal process. Their fears were further reinforced by a lack of confidence in staff around the medications that could be prescribed or the psychosocial advice that could be provided to help reduce the severity of the symptoms of opiate withdrawal. In addition, we were faced with new challenges which included an increased focus on treatment exits, compliance with our payment by results targets, a staff culture that focused singly on maintenance treatment, a service user expectation that engagement in psychosocial interventions was not required, and a general fear of change.

Our greatest challenge during the implementation stage wasour ability to embed this approach as ‘treatment as usual’, alongside the slower reduction or ‘Russian doll’ approach that was more commonly used. Changing culture is often the hardest thing we do in healthcare services and staff engagement in the process was the key to ensuring the approach was owned by the service and offered to service users. To our surprise we achieved this very quickly. Peer mentors were involved from the start and their views adopted into the model; all staff members were trained, and awareness sessions delivered to partnership agencies. Leaflets were placed with all blank care plans, ready for discussion at the service users’ next review appointment.
{kind=link}

For us, it offered a fresh new treatment choice to add to the menu of options for our service users who were looking to make significant behaviour change and improve their lives.
About the authors:
R Iosub and I Seeger are senior registrars, South Gloucestershire and Bristol Specialised Drug and Alcohol Services, Avon and Wiltshire Mental Health Partnership NHS Trust. F D Law is consultant in substance misuse psychiatry at Turning Point. M Gilman is managing director of Discovering Health. N S Wallbank is team manager at Stokes Croft, Bristol Specialised Drug and Alcohol Services, Avon and Wiltshire Mental Health Partnership NHS Trust. J K Melichar is medical director, DHI; medical director, DMT Ltd and consultant in substance misuse psychiatry at Turning Point.